METS医护英语水平考试
全国医护英语水平考试(mets)三级
全国医护英语水平考试(Mets)是由国家卫生健康委员会主管,中国卫生人才网主办的全国性专业英语考试,旨在测试医务人员的英语水平,提高医务人员的英语能力和国际竞争力。
Mets三级考试是该考试的最高级别,主要面向具有一定英语基础的医务工作者。
Mets三级考试主要包括听力、阅读、写作、口语四个部分,考试时间为3小时30分钟。
以下是各个部分的详细介绍:
1. 听力:听力部分共30分钟,包括10个题目,主要测试考生的听力理解能力。
题目形式包括对话、讲座、病例讨论等。
2. 阅读:阅读部分共1小时30分钟,包括15个题目,主要测试考生的阅读理解能力。
题目形式包括文章、图表、图片等。
3. 写作:写作部分共1小时,包括1篇短文和1篇论文,主要测试考生的写作能力。
4. 口语:口语部分共30分钟,包括3个题目,主要测试考生的口语表达能力。
题目形式包括个人陈述、病例讨论、角色扮演等。
Mets三级考试是一项较为综合和难度较大的考试,考生需要在备考过程中注重听力、阅读、写作和口语四个方面的训练和提高。
同时,考生还需要了解考试大纲和考试要求,熟悉考试题型和考试流程,以提高通过考试的机会。
mets医护英语五级考试大纲

mets医护英语五级考试大纲
METS医护英语五级考试大纲包括以下内容:
1. 考试目标:METS医护英语五级考试旨在测试考生在医疗场景下的英语应用能力,包括听力、阅读、写作和口语等方面。
2. 考试内容:考试内容包括医疗场景下的听力、阅读、写作和口语四个部分。
听力部分主要测试考生在医疗场景下的听力理解能力;阅读部分主要测试考生对医疗相关文章的阅读理解能力;写作部分主要测试考生在医疗场景下的英语写作能力;口语部分主要测试考生在医疗场景下的英语表达能力。
3. 考试要求:考生需要通过听力、阅读、写作和口语四个部分的测试,且总分数达到规定的合格线才算通过考试。
具体要求可以根据考试大纲进行查阅。
4. 考试形式:METS医护英语五级考试采用机考的形式进行,考试时间为120分钟。
5. 考试难度:METS医护英语五级考试的难度相对较高,要求考生具备较高的英语水平和医学知识储备。
总之,METS医护英语五级考试大纲是指导考生备考的重要文件,考生需要认真学习和掌握大纲的内容,以提高自己的英语应用能力和通过考试的几率。
全国医护英语水平考试
全国医护英语水平考试(METS)一级复习重点词汇(1)Abdomen腹部1. What is the abdomen breath? 什么是腹式呼吸啊?2. Patients returned home with an ugly and permanent scar on their abdomen.术后病人带着腹部一条丑陋的永久性的疤痕回家了。
Abnormally1. In hemangiomas the endothelial cells multiply at an abnormally rapid rate.在血管瘤中,内皮细胞以非常快的速度进行繁殖。
2. Insulin, a hormone secreted by the pancreas, is a key ingredient in the metabolic process because it helps keep the blood-sugar level from rising abnormally.胰岛素,一种由胰腺分泌的激素,是新陈代谢过程中一种主要的成分,因为它有助于抑制血糖浓度异常地升高。
Absorb1. He was so absorbed in a book that he did not hear the bell. 他如此专心致志地读书以致没听见铃响。
2. Vitamin D helps the body absorb calcium and stimulates bone formation.维生素D能帮助人体吸收钙,刺激骨骼形成。
Ache1. His heart ached for the starving homeless. 他对这忍饥挨饿的无家可归者表示怜悯。
2. Have nerve to ache this symptom? 有没有神经疼痛这个症状?Administration1. Scope: Tax administration. Tax administration. 经营范围:税收管理。
METS医护英语水平考试
1 Introduction to Trauma Care 创伤护理导论2 Patterns of Blunt Injury 钝器损伤的类型3 Mechanisms of Injury /Penetrating Trauma 损伤发病机制/穿透性创伤4 The Physiologic Response to Injury 对损伤的生理学反应5 Shock 休克6 Measurements of Injury Severity 损伤严重程度的测定7 Prehospital Triage 送医院前伤员分类8 Prehospital Therapy 送医院前的治疗9 FieldTeams :Composition,Direction, and Communication with the Trauma Center 现场救护队:组成,指导,与创伤中心的联系10 Air Medical and Interhospital Transport 空中医疗和医院间转运11 Trauma Team Activation 创伤救护队的活动12 Organization prior to Trauma Patient Arrival 创伤病人到达前的组织13 Adult Trauma Resuscitation 成人创伤复苏14 Airway Management in the Trauma Patient 创伤病人的气道处理15 Vascular Access 血管穿刺16 Imaging of Trauma Patients 创伤病人的影像17 Operating Room Practice 手术室常现18 Head Injury 头损伤19 Injuries to the Spinal Cord and Spinal Column 脊髓和脊柱损伤20 Soft Tissue Wounds of the Face 面部软组织伤21 Ophthalmic Injuries 眼损伤22 Penetrating Neck Injury 穿透性颈损伤23 Blunt Neck Injury 颈部钝器损伤24 Thoracic Injury 胸部损伤25 Thoracic Vascular Injury 胸部血管损伤26 Abdominal Injury 腹部损伤27 Abdominal Vascular Injury 腹部血管损伤28 Damage Control 损伤的控制29 Abdominal Compartment Syndrome 腹部隔室综合征30 Genitourinary Injuries 泌尿生殖系统损伤31 Orthopedic Injuries 矫形外科损伤32 Pelvic Fractures 骨盆骨折33 Hand Trauma 手创伤34 Compartment Syndrome and Rhabdomyolysis 隔室综合征和横纹肌溶解35 Peripheral Vascular Injuries 周围血管损伤36 Soft-Tissue Trauma 软组织创伤37 Priorities in the ICU Care of the Adult Trauma Patient 在 ICU 护理的成人创伤病人的优先项目38 Commonly Missed Injuries and Pitfalls 常遗漏的损伤和易犯的错误39 Anesthesia for the Trauma Patient 创伤病人的麻醉40 Trauma Pain Management 创伤疼痛的处理41 Hypothermia, Cold Injury, and Drowning 低温、冷损伤和淹溺42 Blood Transfusion and Complications 输血和并发症43 Nutrition/Metabolism in the Trauma Patient 创伤病人的营养/代谢44 Support of the Organ Donor 器官供体的保养45 Burns /Inhalation 烧伤/吸入46 Pediatric Trauma 儿科创伤47 Care of the Pregnant Trauma Patient 妊娠创伤病人的护理48 Geriatric Trauma 老年人创伤49 Rehabilitation 康复50 Venous Thromboembolism 静脉血栓栓塞51 Injury Prevention 损伤的预防52 House Staff Responsibilities 住院医师的责任53 Legal, Ethical and Family Issues 法律、伦理道德和家庭问题54 Miscellaneous Procedures 各种其它操作程序55 oral health education activity 口腔健康教育活动56 Oral Health Education Unit [Department of Health] 口腔健康教育组57 oral poliomyelitis trivalent 脊灰口服剂58 oral toilet 口腔料理59 oral-maxillofacial surgery and dental unit 口腔颌面外科及牙科部60 outbreak 高峰期;发作;流行61 outbreak control 疫症控制;暴病控制62 outcome management project 医疗成效管理计划63 out-of-pocket expenditure by the user 服务使用者自付64 out-patient appointment system 门诊病人预约制度65 out-patient clinic 门诊诊疗所66 out-patient clinical operations support system 门诊临床运作支持系统67 out-patient consultation service 门诊服务68 out-patient department 门诊部69 out-patient registration system 门诊病人登记制度70 outreach community care programme 外展小区护理计划71 outreach health care team 外展医护队72 outreach medical team 外展医疗队73 outreach specialist medical team 外展专科医疗队86 organic psychosis 器质性精神病87 organoleptic inspection 感官检查88 overall incidence 总发病率89 overflow ward 暂时收容病房;后备病房90 overnight room 夜间当值室91 over-sensitivity 过敏92 ovulation 排卵93 ovulation cycle 排卵周期94 ovulation method 安全期避孕法95 on-call duty doctor 候召当值医生96 oncology 肿瘤学;肿瘤科97 one-way referral 单向转介98 onset of labour 分娩阵痛发作99 onset of symptom 症状发作100 on-site triage treatment 现场分流治疗101 occupational disease 职业病102 occupational health 职业健康103 occupational health nurse 职业健康护士104 Occupational Health Officer 职业健康科医生105 Occupational Hygienist 职业环境生师106 occupational mortality 职业性死亡率107occupational neurosis 职业性神经病108 occupational therapist 职业治疗师109 Occupational Therapists Board 职业治疗师管理委员会110 occupational therapy assessment room 职业治疗评估室111 Occupational Therapy Assistant 职业治疗助理员112 ochlophobia 众恐惧113 ocular pathology 眼科病理学114 ocular prosthesis 假眼115 optimal health 理想的健康状况116 optimum occupancy rate [hospital bed] 最适度病住用率117 optometric assessment 视力测验118 Operations and Training Division [Auxiliary Medical Service Headquarters] 行动及训练部〔医疗辅助队总部〕119 Operations and Training Officer [Auxiliary Medical Service 行动及训练主任〔医疗辅助队〕120 Operations Section [Auxiliary Medical Service Headquarters] 行动组〔医疗辅助队总部〕121 Operations Wing [Auxiliary Medical Service volunteer structure] 行动翼〔医疗辅助队志愿架构〕122 operative treatment 施手术123 oral health care 口腔健康护理;口腔卫生服务124 oral health clinic 口腔卫生诊疗所主任医师(讲课) Professor of Medicine 主任医师(讲课) Professor of Medicine 主任医 师(医疗) Professor of Treatment 儿科主任医师 Professor of Paediatrics 主治医师 Doctor-in-charge 外科主治医师 Surgeon-in-charge 内科主治医师Physician-in-charge 眼科主治医师 Oculist-in-charge 妇科主治医师Gynaecologist-in-charge 牙科主治医师 Dentist-in-charge 医师 Doctor 医士师 Pharmacist 药士 Assistant Pharmacist 主任护师 Professor of Nursing 主管护Nurse 主任技师Technologis 技士Technician Assistant Doctor 主任药师 Professor of Pharmacy 主管药师 Pharmacist-in-charge 药 师 Nurse-in-charge 护师 Nurse Practitioner 护士Technologist 主管技师 Technologist-in-charge 技师SeniorHello, may ( can ) I help you? 您好,我可以帮您吗?What seems to be bothering you? 您觉得哪儿不舒服?Do you have a record? 您有病历吗?I`ll transfer you to the surgery department. 我给您转到外科去what`s wrong with you? 您怎么了?Sit down, please. 请坐。
医护英语水平考试(护理类)考试大纲介绍
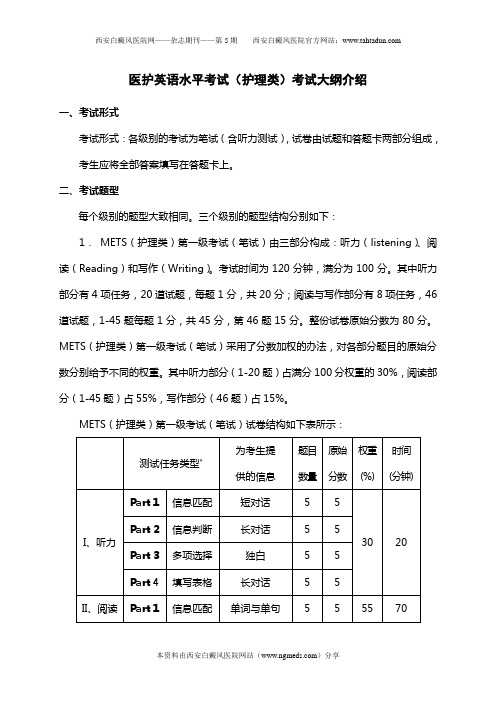
医护英语水平考试(护理类)考试大纲介绍一、考试形式考试形式:各级别的考试为笔试(含听力测试),试卷由试题和答题卡两部分组成,考生应将全部答案填写在答题卡上。
二、考试题型每个级别的题型大致相同。
三个级别的题型结构分别如下:1. METS(护理类)第一级考试(笔试)由三部分构成:听力(listening)、阅读(Reading)和写作(Writing)。
考试时间为120分钟,满分为100分。
其中听力部分有4项任务,20道试题,每题1分,共20分;阅读与写作部分有8项任务,46道试题,1-45题每题1分,共45分,第46题15分。
整份试卷原始分数为80分。
METS(护理类)第一级考试(笔试)采用了分数加权的办法,对各部分题目的原始分数分别给予不同的权重。
其中听力部分(1-20题)占满分100分权重的30%,阅读部分(1-45题)占55%,写作部分(46题)占15%。
METS(护理类)第一级考试(笔试)试卷结构如下表所示:测试任务类型*为考生提供的信息题目数量原始分数权重(%)时间(分钟)I、听力Part 1信息匹配短对话 5 530 20 Part 2信息判断长对话 5 5Part 3多项选择独白 5 5Part 4填写表格长对话 5 5II、阅读与写作Part 1信息匹配单词与单句 5 555 70 Part 2信息匹配单句与告示 5 5Part 3 信息匹配单句与图表 5 5Part 4 补全对话长对话与单句 5 5Part 5 多项选择单句7 7Part 6 信息判断短文8 8Part 7 完形填空短文10 10Part 8短文写作表格 1 15 15 30总计65+1 80 100 120 *实际考试中卷中可能会出现新任务类型2. METS(护理类)第二级考试(笔试)由三部分构成:听力(listening)、阅读(Reading)和写作(Writing)。
考试时间为120分钟,满分为100分。
医护英语水平考试METS(护理类)模拟试题集
目录医护英语水平考试(护理类)第一级模拟试题 ................................................. 错误!未定义书签。
医护英语水平考试(护理类)第二级模拟试题 ................................................. 错误!未定义书签。
医护英语水平考试(护理类)第三级模拟试题 ................................................. 错误!未定义书签。
医护英语水平考试(护理类)第一级模拟试题2010 年6 月METS 模拟试题医护英语水平考试(护理类)第一级Medical English Test System (METS)(For Nurses)Level 1姓名准考证号时间:120 分钟考生注意事项1.严格遵守考场规则,考生得到监考人员指令后方可开始答题。
2.答题前考生须将自己的姓名和准考证号写在试卷和答题卡上。
3.答客观题时,一律用2B 铅笔,按照答题卡上的要求答题。
如要改动答案,必须用橡皮擦干净。
4.答翻译与写作题时,必须用黑色签字笔在答题卡上答题。
5.注意字迹清楚,保持卷面整洁。
6.考试结束时将试卷和答题卡放在桌上,不得带走。
待监考人员收毕清点后,方可离场。
※ 未经批准,本试卷任何单位或个人不得保留、复制和出版,违者必究。
医护英语水平考试办公室第一部分听力理解(20% )( 20分钟)第一节选择填空在本节中,你将听到10 个句子,每个句子后有三个选项,根据你所听到的录音,从试卷中所给的[ A] 、[B] 、[C]三个选项中选出正确答案填入句子空白处,并在答题卡上将相应字母涂黑。
每个句子读两遍。
例如,你将听到以下内容:I ' ve goatn awful pain in my belly.请看选项:I ' ve goatn awful pain in my _______ .[A] joints [B] armpit [C] belly根据你所听到的录音,答案应选[C] 项。
mets医学英语水平考试
mets医学英语水平考试
METS即医学英语水平考试(Medical English Test System),是由国
家卫生健康委人才交流服务中心和中国教育国际交流协会联合举办的,面向我国医药卫生人才的全国性专业英语考试项目。
该考试标准的设立是根据我国医院实际工作需要,重点考查应试人员在医疗环境下熟练运用专业语言进行学习和工作的能力。
METS考试旨在促进就业,考查考生的医护专业外语的实际应用能力,为
医护人员提供专业英语能力的证明,为用人单位录用和考核员工提供参考依据。
该考试不仅适合医护技专业学生、医药护技行业从业人员,也适合医学英语教师、医学英语兴趣爱好者等人群参加。
医护英语水平考试(METS)三级样题及答案
医护英语水平考试第三级Medical English Test System (METS)Level 3姓名__________ 准考证号__________ 时间:120分钟考生须知13.严格遵守考场规则,考生得到监考人员指令后方可开始答题。
14.答题前考生须将自己的姓名和准考证号写在试卷和答题卡上。
15.答客观题时,一律用2B铅笔,按照答题卡上的要求答题。
如要改动答案,必须用橡皮擦干净。
16.答写作题时,必须用黑色签字笔在答题卡上答题。
17.注意字迹清楚,保持卷面整洁。
18.考试结束时将试卷和答题卡放在桌上,不得带走。
待监考人员收毕清点后,方可离场。
===================================================I ListeningPart 1Questions 1 – 5• You will hear five extracts from conversations in different clinical departments.•For questions 1-5, choose from the list A-F to show which case each doctor is talking about. Use the letters only once. There is one extra letter which you do not need to use.•You will hear each recording twice.Doctor 1 Doctor 2 Doctor 3 Doctor 4 Doctor 5 A The patient has difficulty in coughing up phlegm.BThe patient ‘s got some lumps of fibrous tissue on the womb which are causing the bleeding.CThe patient ‘s family members are prone to develop gastroesophageal reflux problem.DThe patient needs some treatments to prevent further deterioration of the kidney illness.E The patient has to be hospitalized and isolated.F The patient had better choose a non-surgical treatment for his condition.Questions 6 – 13•You will hear a conversation between two doctors.•Are the following statements ―R ight‖ or ―W rong‖? If there is not enough information to answer ―R ight‖ or ―W rong‖, choose ―Not Menti oned.‖•You will hear the recording twice.6 Dr. Harry Drabkin is an expert who has been carrying out enterological research.A RightB WrongC Not Mentioned7 There are nearly 40,000 people who develop kidney cancer in the U. S. every year.A RightB WrongC Not Mentioned8 With kidney cancer, back pain and blood in the urine are the common symptomsoccurring at the early stage.A RightB WrongC Not Mentioned9 Small tumors in the kidney tend to be benign.A RightB WrongC Not Mentioned10 Spots in the lung may suggest late tumors of the kidney.A RightB WrongC Not Mentioned11 Visible blood in the urine can also signal other diseases but does not require animmediate visit to the doctor.A RightB WrongC Not Mentioned12 Laparoscopic-based operation on small tumors involves long and midline incision.A RightB WrongC Not Mentioned13 Tumors at more advanced stage as well as early tumors can be removed bylaparoscopic surgery.A RightB WrongC Not MentionedQuestions 14 – 20•You will hear a discussion among a supervising physician and two medical students. •For questions 14-20, choose the best answer.•You will hear the discussion twice.14 Clinton developed aA gastric disease.B cardiovascular disease.C renal disease.15 Clinton‘s disease was treated byA acupuncture.B chemotherapy.C surgery.16 Clinton had experienced the following exceptA angina.B heartburn.C tightness in the chest.17 Which is not the risk factor for coronary heart disease?A Fatigue.B Hypertension.C Heredity.18 Doughnut isA a vegetable containing lots of fiber.B a high-calorie snack.C a delicious fruit rich in vitamin C.19 What lesson can be drawn from Clinton case?A Public figures should inform the people of their illness.B Patients should undergo annual screening test.C Patients can halt the drug if there is improvement.20 Which of the following statements about Clinton is true?A Clinton underwent high standard medical screening test every year.B Clinton always followed the doctor‘s advice.C An unhealthy diet was mainly responsible for Clinton‘s disease.Questions 21 – 25●You will hear a speech on the killer American diet that‘s sweeping the world.•For questions 21–25, complete the notes. In each space write only one word. •You will hear the speech twice.Notes:the (21) …………… of cardiovascular disease, diabetes, hypertension, preventable by changing diet and lifestyleglobal illness examples:●Asia (from having one of the lowest rates of heart disease, obesity anddiabetes to one of the highest)●Africa (cardiovascular disease equals the HIV and AIDS death)make a difference in diet and practice (22) …………… medicine on a global scale●heart and blood vessel disease still kill more people, preventable and(23) ……………●prostate cancer, progression stopped and reversed, 70 percent regressionor (24) …………… of tumor growth●diabetes, two thirds of adults and 15 percent of kids, increased 70 percent inthe past 10 years, pitiful and preventablewhat we can do●an Asian diet can reverse heart disease and cancer●work with big food companies (McDonald's,and PepsiCo, and ConAgra), makean Asian salad, two-thirds revenue from better foods●free up resources for drugs, treat AIDS, HIV and malaria, prevent(25) …………… flu.II ReadingPart 1Questions 1 – 10•Read the following article about young athletes‘ sport injuries.•For questions 1–5, choose the most suitable heading from the list A–F for each part (1–5) of the article. For questions 6–10, choose the best answer for each space from the list A–F for each sentence (6–10).•Mark the correct letter A–F on your answer sheet.Young Athletes: Injuries and Prevention1High profile events like the Olympics bring the hope that witnessing and celebrating dedicated athletes at the top of their game, will inspire young people to take up sport and physical activities that help them develop confidence, lead more satisfying lives, and not least, secure long-term health by reducing their risk for developing chronic illness like diabetes, obesity, cancer and cardiovascular diseases.But unfortunately, if they don't take appropriate measures, young athletes can instead, end up in pain, on a different path to poor health, due to avoidable sport injury.2According to the National Institute of Arthritis and Musculoskeletal and Skin Diseases, which is part of the National Institutes of Health in the US, the most common sport injuries are due to accidents, poor training practices or using the wrong gear or equipment. People can also hurt themselves because they are not in shape or because they don't warm up or stretch enough. Some injury experts in the US have said they are also seeing more and more young athletes injured because of overuse and doing too much, and this may partially explain the growing numbers that drop out of sport by the eighth grade. The most common sport injuries are: knee injuries, sprains and strains, swollen muscles, Achilles tendon injuries, pain along the shin bone, and fractures and dislocations. 3Prehabilitation, is a relatively new idea in sports medicine and therapy. It is a personalized exercise program that is individually designed for athletes to help them prevent injury in their given sport. The aim of prehab is to avoid injury by compensating for the repetitive movements and stresses of regular, often daily, training. In some respects, you can view athletic training for peak performance in a sport as a form of repetitive strain, with the potential to result in injury in much the same way as computer operators can get occupational injuries like carpal tunnel syndrome and shoulder problems. With repetitive use, muscles become tight, the body develops imbalances in strength and muscle coordination. These happen naturally during activity, but because training is repetitive, they become repeatedly reinforced with each workout, unless that workout also incorporates some compensating activity, such as in a prehab routine.4To ensure the best chance of success with prehab, the athlete should start practising it before injury occurs. But unfortunately the usual route to prehab is via injury. A typical scenario is the athlete injures him or herself, goes to a sport therapist or specialist trainer for rehabilitation (rehab), and the therapist then persuades them to sign up for prehab to stop it happening again. Another way to keep prehab useful and working for the athlete, is to ensure it continually evolves with the needs and changing fitness and ability of the individual. The exercises should be progressive and re-evaluated regularly. There is also the important need to challenge and motivate the athlete, and stop them becoming bored, or habituated to the program.5 A successful prehab program is one that forms a regular part of an athlete's training routine. The therapist needs to have a detailed knowledge of the athlete's sport, theirstrengths and weaknesses, and be able to have frank, open conversations with the individual.1 Paragraph 1 _____2 Paragraph 2 _____3 Paragraph 3 _____4 Paragraph 4 _____5 Paragraph 5 _____6 If they don't take appropriate measures, young athletes can end up in pain due toavoidable __________.7 More and more young athlete injuries may partially explain the __________ that dropout of sport by the eighth grade.8 The aim of prehab is to avoid injury by compensating for the __________ andstresses of regular, often daily, training.9 The athlete injures him or herself, goes to a sport therapist or specialist trainer for__________.10 A successful prehab program should form a regular part of an athlete's __________.A extreme limitsB sport injuryC growing numbersD rehabilitationE training routineF repetitive movementsPart 2Questions 11 – 17•Read the following article about life of student doctors.•For questions 11–17, choose the answer (A, B, C or D)which you think fits best according to the text.•Mark your answers on the answer sheet.Student DoctorsIn comparison with the lives of other postgraduate students, the life of a student doctor is far from easy. Despite the heavy workload, it seems that the more you learn, the more you realize what you still need to study. As a result, it is not unusual for students to drop out. Misguided teachers attempt to simplify matters in an environment that demands the very best of its practitioners.The situation is little better in the year or two years after qualifying. Poorly paid for such long hours, many junior doctors find themselves becoming disillusioned with medicine. The more depressed they become, the more likely they are to look elsewhere for a career, wasting up to sever years of training and education. An unfortunate statistic is that of those that qualify as doctors, 18% do not remain in the profession for more than three years.The problem can be more clearly defined by considering specific examples. In New Zealand and Britain, for example, the exodus of medical graduates is leaving the remaining newly qualified doctors with responsibilities that are beyond their capacity. In statistics from 1998 over half the graduates from one medical school in New Zealand left the country immediately after qualifying, and hospitals are really beginning to feel the shortage. Certain hospitals in Auckland, for example, do not have enough staff to cover the timetable, and some of the newly qualified doctors are finding themselves on call for 48 hours straight. In Britain, the situation is equally bleak.The structure of the health service itself is the most important factor to be taken into account when considering the number of migrating British medical graduates. Junior doctors are required to take mentors, more senior doctors (often consultants), to act as supervisors. They are entrusted with the educational supervision of doctors in their first year of practice and are responsible for ensuring the application of the principles of good medical practice. However, when interviewed, slightly less than 60% of junior doctors had any positive feedback on the relationship. The remaining respondents described situations in which a consultant was accused of making unreasonable demands, bullying, being unfair, or being sexist. In more extreme cases, the consultant was portrayed as incompetent, insensitive or negligent towards patients.In New Zealand, the situation, although having essentially the same effect of fewer junior doctors, has different causes. There are two main factors which explain this mass migration of medical graduates from New Zealand. The first factor is the student loans system where a medical graduate can leave university having accumulated a loan of anything up to NZ$60,000 in the course of training. By leaving the country, such graduates have the option of at least delaying the repayment of those loans. The other reason is the long hours. The stories of working hours a week being almost in the three-figure mark are often not exaggerated, and this is a situation which is worsening the fewer junior doctors there are.11 The reasons why some student doctors don‘t want to remain in their professioninclude all the following except _________.A heavy workloadB high demand of the professionC being poorly paidD no chance for career development12 According to the passage, teachers of student doctors _________ the complexity oftheir living condition.A overestimateB underestimateC know exactlyD ignore13 For student doctors, which of the following is not true?A Medical courses are more difficult than many other postgraduate courses.B The more they learn, the more they realize what they still need to learn.C A number of graduates are not remaining in the medical field.D Once qualified, the situation for junior doctors slightly improves.14 What does the word ―exodus‖ (Line 2, in the 2nd sentence of the 3rd paragraph) mean?A Declaration.B Expression.C Departure.D Deduction.15 What is the main factor for the migrating of student doctors in Britain?A The structure of the health service.B Full work timetable.C Dissatisfaction with their mentors.D Incompetence for their work.16 According to the interview, _________ student doctors had nothing positive to sayabout their mentors.A slightly less than 60%B slightly more than 60%C slightly less than 40%D slightly more than 40%17 The root of the problem in New Zealand and Britain is _________.A essentially the sameB similarC quite differentD analogousPart 3Questions 18 – 25•Read the following article on the organization, Doctors Without Borders.•Are sentences 18–25on the next page ―Right‖ or ―Wrong‖? If there is not enough information to answer ―Right‖ or ―Wrong‖, choose ―Not Mentioned‖.•For each sentence 18–25, mark one letter A–C on your answer sheet.Doctors Without BordersDoctors Without Borders, French Médecins Sans Frontières (MSF), is an international humanitarian group dedicated to providing medical care to victims of political violence or natural disasters, as well as to those who lack access to such treatment. The group was awarded the 1999 Nobel Prize for Peace.Doctors Without Borders was founded in 1971 by 10 French physicians who were dissatisfied with the neutrality of the Red Cross. The doctors believed they had the right to intervene wherever they saw a need for their assistance, rather than waiting for an invitation from the government, and they also felt they had a duty to speak out about injustice, even though it might offend the host government. In 1972 Doctors Without Borders conducted its first major relief effort, helping victims of an earthquake in Nicaragua. Other significant missions were undertaken to care for victims of fighting in Lebanon (1976), and Afghanistan (1979). Doctors Without Borders has continued to work to relieve famine, offer medical care to casualties of war, and deal with the problem of refugees in many countries throughout the world. In 2003 Doctors Without Borders was a founding partner in the organization Drugs for Neglected Diseases Initiative (DNDi), which works to create medicines for such diseases as malaria, tuberculosis, and HIV/AIDS.Doctors Without Borders works in more than 70 countries. Headquartered in Brussels, the organization has offices in some 20 countries. It was an integral part of the emergency relief efforts in Haiti after the earthquake of 2010, though all three of the organization‘s hospitals in that country had been destroyed by the quake.In addition to providing medical assistance, Doctors Without Borders has a reputation as a highly politicized group, particularly skillful in achieving publicity for its efforts. Its vocal opposition to perceived injustice led to its expulsion from several countries.Doctors Without Borders is a neutral and impartial humanitarian organization that aims first and foremost to provide high-quality medical care to the people who need it the most. It does not promote the agenda of any country, political party, or religious faith, and, as such, endeavors to communicate its history, background, and capabilities to all parties in a given situation so that it may gain the necessary access to populations in need. ―It is saving a lot of people–children and adults–who might otherwise have died, from malnutrition or from preventable causes. There are no other agencies anywhere near here, and we are the only organization providing assistance–in terms of both health care and food–in this region. We have been doing this for years.‖18 Doctors Without Borders is a governmental organization, known for its continuousefforts in providing medical care around the world.A RightB WrongC Not Mentioned19 Doctors Without Borders believes that all people have the right to medical careregardless of race, religion, creed or political affiliation.A RightB WrongC Not Mentioned20 Doctors Without Borders was once a branch of the Red Cross, but later cut its tieswith it because of financial problems.A RightB WrongC Not Mentioned21 Doctors Without Borders was founded in Paris, France in 1971. Its principles aredescribed in the organization's founding charter.A RightB WrongC Not Mentioned22 The first major mission conducted by Doctors Without Borders were to care forvictims of fighting in Nicaragua.A RightB WrongC Not Mentioned23 Doctors Without Borders, headquartered in Brussels, has offices in more than 70countries.A RightB WrongC Not Mentioned24 Because all three of the organization‘s hospitals in Haiti had been destroyed by thequake of 2010, Doctors Without Borders failed to give medical relief.A RightB WrongC Not Mentioned25 As a highly politicized group, Doctors Without Borders is not welcomed by allcountries.A RightB WrongC Not MentionedPart 4Questions 26 – 30•Read the following text about sadness. Five sentences have been removed from the article.•Choose from the sentences A–F the one which fits each space (26–30). There is one extra sentence which you do not need to use.•For each space (26–30), mark one letter A–F on your answer sheet.When Sadness Is a Good ThingIn the 1960s, the pharmaceutical company Sandoz marketed its new tranquilizer Serentil with ads in medical journals suggesting the drug be prescribed to ―the newcomer in town who can't make friends, the woman who can't get along with her new daughter-in-law or the executive who can't accept retirement.‖ But the FDA stopped the ads. Drugs are supposed to treat illnesses, the agency said, not the vicissitudes of living.Isn't that a quaint idea?(26)…………….But today 7% of Americans are on antidepressants (many more have tried them), and ads have touted the drugs for ordinary problems like fatigue, loneliness and sadness. Still, drug companies aren't the (sole) villain in this story. As Allan Horwitz and Jerome Wake-field point out in their incisive new book.The Loss of Sadness: How Psychiatry Transformed Normal Sorrow into Depressive Disorder, we now have a ―legal drug culture‖ built around the widely accepted idea that feeling blue is an illness.Horwitz, dean of social and behavioral sciences at Rutgers, and Wakefield, an expert on mental-illness diagnosis at New York University, agree that depression can have biological roots. (27)……………. They also point out that the human capacity to feel sad is an evolutionarily selected trait that we might not want to drug away.We've been living in an age of melancholy for at least two decades. Outpatient treatment of depression rose 300% between 1987 and 1997. But while it‘s tempting to blame our culture—fear of terrorists, too much caffeine, living by BlackBerry—there's a more straightforward explanation for the boom in dejection. In 1980 the American Psychiatric Association published a new definition of depression in the Diagnostic and Statistical Manual of Mental Disorders—usually shortened to DSM—the compendium used by mental-health professionals to make diagnoses.(28)……………The much longer 1980 definition (which is still used, with slight modifications) omitted the requirement that symptoms be ―excessive‖ in proportion to cause. In fact, the revised manual said nothing about causes and listed symptoms instead.To be diagnosed with major depressive disorder today, you need have only five symptoms for two weeks, which can include such common problems as depressed mood, weight gain, insomnia, fatigue and indecisiveness. The DSM does make an exception for bereavement: if you recently lost a loved one, such symptoms are not considered disordered. But the manual doesn't make exceptions for other things that make us sad—divorce, financial stress, a life-threatening illness.Still, is there anything wrong with medicating normal sadness if you don't mind side effects? Horwitz and Wakefield take no position on this.(29)……………But the authors also note that ―loss responses are part of our biolog ical heritage‖. Nonhuman primates separated from sexual partners or peers have physiological responses that correlate with sadness, including higher levels of certain hormones. Human infants express despair to evoke sympathy from others.(30)……………It also teaches us that whatever prompted the sadness—say, getting fired because you were always late to work—is behavior to be avoided. This is a brutal economic approach to the mind, but it makes sense: we are sometimes meant to suffer emotional pain so that we will make better choices.A These sadness responses suggest sorrow is genetic and that it is useful attracting socialsupport, protecting us from aggressors.B The FDA was worried back then about an overmedicated society; in 1956, 5 % ofAmericans were on tranquilizers.C But they persuasively argue that many instances of normal sadness—the kind thatdescends after you lose a job or get dumped—are now misdiagnosed as depressive disorder.D The new definition was a radical departure from the old one, which had described―depressive neurosis‖ as ―an excessive reaction of depression due to an internal conflict or to an identifiable event such as the loss of a love object.‖E If you struggle with constipation or diarrhea, something is wrong and you are contributing tothe toxic overload and poisoning of your body.F They point out that women giving birth take painkillers even though pain is a normal part ofthe process.Part 5Questions 31 – 40•Read the following text on administering medications.•Choose the best word (A, B, C or D) for each space.•For each space 31–40, mark one letter A–D on your answer sheet.31A over B beyond C through D on32A desired B great C contrast D fast33A additive B placebo C contrary D adverse34A for B as C with D on35A as B through C against D for36A commission B omission C emissions D transmission 37A Because B Whereas C Although D Despite38A frequently B consequently C definitely D undoubtedly 39A conscious B ignoring C neglecting D aware40A refined B dominated C noticed D definedIII WritingQuestion 41●Write an essa y of about 150 words on the topic ―Should Doctors and Nurses Lie?‖ You shouldbase your essay on the clues given below.●Please write your essay on the Answer Sheet.Should Doctors and Nurses Lie?1. 医生、护士向绝症病人撒谎隐瞒病情的现象很常见2. 但有些医生护士对此持反对观点3. 你的看法METS第三级考试听力录音文本This is METS 3 Listening Test.There are four parts in the test. Parts One, Two, Three, and Four.You will hear each part twice.We will now stop for a moment before we start the test.Please ask any questions now because you must not speak during the test.Pause (10 seconds)Now, look at the instructions for Part One.Pause (3 seconds)You will hear five extracts from conversations in different clinical departments.For questions 1-5, choose from the list A-F to show which case each doctor is talking about. Use the letter only once. There is one extra letter which you do not need to use. You will hear each recording twice.Pause (3 seconds)Now we are ready to start.Pause (3 seconds)Conversation 1Hello, Mr. Hartley. Come and sit down. The tests show that it is probably a condition called chronic glomerulonephritis which has damaged the kidney. The condition is irreversible – nothing can be done to put it right at this stage I‘m afraid. You‘ve undoubtedly had it for a long time. We‘ll need to keep an eye on you. There are fortunately treatments to make up for the kidney damage.Pause (30 seconds)Conversation 2Well, the X-ray doctor found irritability and distortion of the duodenum although there was no actual ulcer visible on the X-ray. This does not necessarily mean that you have no ulcer. We have to decide the best way of treating it. There are two ways: medical and surgical. In young people we try to avoid operations and we hope that medical means will help. There is no risk attached to the operation and most patients get better after it and have no side effects. But with young people we usually persist with medical treatment.Pause (30 seconds)Conversation 3I can‘t find anything seriously wrong with you. I think this is due to the weakness of the muscle at the lower end of your gullet which is allowing acid to come back into your gullet. We‘d better do an X-ray of the stomach and gallbladder as you have this tendency in your family. We‘ll check on the blood as well. Avoid bending. The stomach should not be empty of food for too long. Try to eat little and often. I‘ll give you some medicine to take after meals. I‘ll see you in three weeks when I‘ve got the results of the X-rays and tests.Pause (30 seconds)Conversation 4Well, one of these would clear the chest in the morning. All you do is shake it and puff. One puff isusually sufficient. You must not have more than two puffs and no more for three hours. These are absolutely safe if you stick to that dose. This would help to clear your chest and before you go up a hill you could have a puff. I‘ll write to your doctor about that, shall I?Pause (30 seconds)Conversation 5It‘s difficult to say just now exactly what‘s wrong. Try to relax and keep calm. Now I would like to transfer you to the Isolated Ward. Please wait until we get the result of the blood test and the X-ray. If you are suffering from SARS indeed, you will be all right after proper treatment in most conditions, although the process may be slow.Pause (30 seconds)Now you’ll hear Part 1 again.This is the end of Part OnePause (3 seconds)Now look at Part Two.You will hear a conversation between two doctors.Are the following statements “R ight” or “W rong”? If there is not enough infor mation to answer “R ight” or “W rong”, choose “Not M entioned.”You will hear the recording twice.Pause (3 seconds)Doctor A: I am Dr. Linda Austin. I am interviewing Dr. Harry Drabkin who is the Chief of Hematology-Oncology here at the Medical University of South Carolina. Dr.Drabkin, I know that your own area of specialty is in kidney cancer, or renalcancer. How common is that cancer?Doctor B: Approximately, I would say, 35,000 to 38,000 cases in the U.S. every year. And it tends to be a fairly silent disease. It is an internal organ. It is not something thatyou feel getting bigger. Most people have fairly no symptoms with early disease.The symptoms they develop are usually late, things like back pain. Blood in theurine, I would say, probably is one of the more common things for late diseases,when the tumors are large. Many tumors today are discovered incidentallybecause of a CT scan that was done for some other reason. It is a greattechnique. It is very accurate. We are picking up more and more small tumors.Those tumors, by and large, tend to be not metastatic. So, the ones that I see,that have spread to some place else, like the lung, or bones, or liver, or someplace like that, are these late tumors. It is much like ovarian cancer in terms of notproducing symptoms until it is very late.Doctor A:So I guess one take-home point, then, is anytime one has visible blood in the urine, it certainly is time to call your doctor right away.Doctor B:Absolutely. And it doesn‘t have to be kidney cancer. It could be a bladder infection. It could be a stone in the bladder. It could be a tumor somewhere in thesystem from the bladder to the ureters, to the kidney, whatever. But the importantthing is, it should never be left alone, always should be looked at.Doctor A:You mentioned that often these tumors are picked up incidentally. The doctor may have ordered a scan for something else and sees a small tumorin the kidney that has not spread. In that case, is it a pretty simple matter ofjust operating on it?Doctor B:It is a simple matter. And the surgery these days for small tumors is pretty simple.For the most part, it can be laparoscopic-based. So, instead of having a bigincision, you have a couple of small holes in your belly where the surgeons go in,stick the scopes, fill the belly up with air and take these tumors out. People are out。
医护英语(METS)水平考试大纲
目录一、考试性质 (1)二、考试用途 (1)三、等级标准 (1)四、考试内容及要求 (3)(一)医护英语水平考试第一级考试内容及要求 (3)(二)医护英语水平考试第二级考试内容及要求 (8)(三)医护英语水平考试第三级考试内容及要求 (13)(四)医护英语水平考试第四级考试内容及要求 (18)五、考试样题及答案 (24)(一)医护英语水平考试第一级考试样题及答案 (24)(二)医护英语水平考试第二级考试样题及答案 (42)(三)医护英语水平考试第三级考试样题及答案 (64)(四)医护英语水平考试第四级考试样题及答案 (86)六、医护英语词汇表 (112)(一)医护英语水平考试第一级考试词汇表 (112)(二)医护英语水平考试第二级考试词汇表 (128)(三)医护英语水平考试第三级考试词汇表 (152)(四)医护英语水平考试第四级考试词汇表 (185)一、考试性质医护英语水平考试(Medical English Test System,以下简称METS)是为我国各类医药卫生院校学生和医药卫生行业从业人员开发设计的一项社会化英语水平考试,旨在考查应考人员在医学环境下的英语实际应用水平,属于非学历标准参照性考试。
二、考试用途作为一套针对医药卫生行业工作环境开发的英语水平考试系统,METS重点考查应考人员的英语实际应用能力,是医药卫生院校学生评价自己英语水平和求职就业的重要参考,是医药卫生部门招聘员工评估其英语能力的可靠标准,是各单位人力资源部门提升或调配员工以及制定人力资源解决方案的重要依据。
三、等级标准METS的考试级别设置为一级、二级、三级、四级;一级为初始级,四级为最高级。
级别的设定充分考虑了我国医药卫生类院校的英语教学状况和医药卫生专业技术人员的英语水平,同时也参考了国内外有影响的标准化考试,如CET-4、CET-6、PETS、TOEFL、IELTS、CEFR(Common European Framework of Reference for Languages: Learning,Teaching, Assessment“欧洲语言教学共同纲领”)等。
医护英语水平考试(METS)四级样题试卷及答案
I LISTENING
Part 1
Questions 1 – 10
Questions 1-5 Choose the correct answer, A, B or C.
1 What is a stroke? A It is a loss of blood flow in the brain. B It is a loss of blood flow in the heart. C It is a loss of blood flow in the extremities.
Physical examination: (18) __________ abdomen and icteric sclerae Personal history: no contact with toxic chemicals or clear-water streams, heavy (19) __________ intake of five years’ duration
situation in a couple of other countries
Subjects of the research people under 18 should be excluded focus on men who were in (32) _______________ people who didn‘t have jobs and employed women as a separate (33)
Problems encountered in collecting data a person shopping in town decided to (37) _______________ when it came to the
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
1 Introduction to Trauma Care 创伤护理导论2 Patterns of Blunt Injury 钝器损伤的类型3 Mechanisms of Injury/Penetrating Trauma 损伤发病机制/穿透性创伤4 The Physiologic Response to Injury 对损伤的生理学反应5 Shock 休克6 Measurements of Injury Severity 损伤严重程度的测定7 Prehospital Triage 送医院前伤员分类8 Prehospital Therapy 送医院前的治疗9 Field Teams:Composition,Direction, and Communication with the Trauma Center 现场救护队:组成,指导,与创伤中心的联系10 Air Medical and Interhospital Transport 空中医疗和医院间转运11 Trauma Team Activation 创伤救护队的活动12 Organization prior to Trauma Patient Arrival 创伤病人到达前的组织13 Adult Trauma Resuscitation 成人创伤复苏14 Airway Management in the Trauma Patient 创伤病人的气道处理15 Vascular Access 血管穿刺16 Imaging of Trauma Patients 创伤病人的影像17 Operating Room Practice 手术室常现18 Head Injury 头损伤19 Injuries to the Spinal Cord and Spinal Column 脊髓和脊柱损伤20 Soft Tissue Wounds of the Face 面部软组织伤21 Ophthalmic Injuries 眼损伤22 Penetrating Neck Injury 穿透性颈损伤23 Blunt Neck Injury 颈部钝器损伤24 Thoracic Injury 胸部损伤25 Thoracic Vascular Injury 胸部血管损伤26 Abdominal Injury 腹部损伤27 Abdominal Vascular Injury 腹部血管损伤28 Damage Control 损伤的控制29 Abdominal Compartment Syndrome 腹部隔室综合征30 Genitourinary Injuries 泌尿生殖系统损伤31 Orthopedic Injuries 矫形外科损伤32 Pelvic Fractures 骨盆骨折33 Hand Trauma 手创伤34 Compartment Syndrome and Rhabdomyolysis 隔室综合征和横纹肌溶解35 Peripheral Vascular Injuries 周围血管损伤36 Soft-Tissue Trauma 软组织创伤37 Priorities in the ICU Care of the Adult Trauma Patient 在ICU护理的成人创伤病人的优先项目38 Commonly Missed Injuries and Pitfalls 常遗漏的损伤和易犯的错误39 Anesthesia for the Trauma Patient 创伤病人的麻醉40 Trauma Pain Management 创伤疼痛的处理41 Hypothermia,Cold Injury,and Drowning 低温、冷损伤和淹溺42 Blood Transfusion and Complications 输血和并发症43 Nutrition/Metabolism in the Trauma Patient 创伤病人的营养/代谢44 Support of the Organ Donor 器官供体的保养45 Burns/Inhalation 烧伤/吸入46 Pediatric Trauma 儿科创伤47 Care of the Pregnant Trauma Patient 妊娠创伤病人的护理48 Geriatric Trauma 老年人创伤49 Rehabilitation 康复50 Venous Thromboembolism 静脉血栓栓塞51 Injury Prevention 损伤的预防52 House Staff Responsibilities 住院医师的责任53 Legal,Ethical and Family Issues 法律、伦理道德和家庭问题54 Miscellaneous Procedures 各种其它操作程序55 oral health education activity口腔健康教育活动56 Oral Health Education Unit [Department of Health]口腔健康教育组57 oral poliomyelitis trivalent 脊灰口服剂58 oral toilet 口腔料理59 oral-maxillofacial surgery and dental unit口腔颌面外科及牙科部60 outbreak高峰期;发作;流行61 outbreak control疫症控制;暴病控制62 outcome management project 医疗成效管理计划63 out-of-pocket expenditure by the user服务使用者自付64 out-patient appointment system门诊病人预约制度65 out-patient clinic门诊诊疗所66 out-patient clinical operations support system门诊临床运作支持系统67 out-patient consultation service门诊服务68 out-patient department门诊部69 out-patient registration system门诊病人登记制度70 outreach community care programme外展小区护理计划71 outreach health care team外展医护队72 outreach medical team外展医疗队73 outreach specialist medical team外展专科医疗队74 outside appointment book出外就医册75 ordinary diet普通膳食76 organ donation器官捐赠77 Organ Donation Card器官捐赠证78 Organ Donation Centre器官捐赠中心79 organ donation form 器官捐赠表格80 Organ Donation Register [Hong Kong Medical Association] 器官捐赠册81 organ donor 器官捐赠人82 organ imaging器官造影83 organ pledge 承诺捐出的器官数目84 organ recipient器官受赠人85 organ transplant器官移植86 organic psychosis器质性精神病87 organoleptic inspection感官检查88 overall incidence总发病率89 overflow ward暂时收容病房;后备病房90 overnight room夜间当值室91 over-sensitivity过敏92 ovulation排卵93 ovulation cycle排卵周期94 ovulation method安全期避孕法95 on-call duty doctor候召当值医生96 oncology肿瘤学;肿瘤科97 one-way referral单向转介98 onset of labour分娩阵痛发作99 onset of symptom症状发作100 on-site triage treatment现场分流治疗101 occupational disease职业病102 occupational health 职业健康103 occupational health nurse职业健康护士104 Occupational Health Officer 职业健康科医生105 Occupational Hygienist职业环境生师106 occupational mortality职业性死亡率107occupational neurosis职业性神经病108 occupational therapist职业治疗师109 Occupational Therapists Board职业治疗师管理委员会110 occupational therapy assessment room职业治疗评估室111 Occupational Therapy Assistant职业治疗助理员112 ochlophobia 众恐惧113 ocular pathology眼科病理学114 ocular prosthesis假眼115 optimal health理想的健康状况116 optimum occupancy rate [hospital bed]最适度病住用率117 optometric assessment视力测验118 Operations and Training Division [Auxiliary Medical Service Headquarters] 行动及训练部〔医疗辅助队总部〕119 Operations and Training Officer [Auxiliary Medical Service行动及训练主任〔医疗辅助队〕120 Operations Section [Auxiliary Medical Service Headquarters] 行动组〔医疗辅助队总部〕121 Operations Wing [Auxiliary Medical Service volunteer structure]行动翼〔医疗辅助队志愿架构〕122 operative treatment 施手术123 oral health care口腔健康护理;口腔卫生服务124 oral health clinic口腔卫生诊疗所主任医师(讲课) Professor of Medicine主任医师(讲课) Professor of Medicine主任医师(医疗) Professor of Treatment儿科主任医师Professor of Paediatrics主治医师Doctor-in-charge外科主治医师Surgeon-in-charge内科主治医师Physician-in-charge眼科主治医师Oculist-in-charge妇科主治医师Gynaecologist-in-charge牙科主治医师Dentist-in-charge医师Doctor医士Assistant Doctor主任药师Professor of Pharmacy主管药师Pharmacist-in-charge药师Pharmacist药士Assistant Pharmacist主任护师Professor of Nursing主管护师Nurse-in-charge护师Nurse Practitioner护士Nurse主任技师Senior Technologist主管技师Technologist-in-charge技师Technologis技士TechnicianHello, may (can)I help you? 您好,我可以帮您吗?What seems to be bothering you? 您觉得哪儿不舒服?Do you have a record? 您有病历吗?I`ll transfer you to the surgery department. 我给您转到外科去what`s wrong with you? 您怎么了?Sit down,please. 请坐。