艾塞那肽说明书
阿斯利康Bydureon(艾塞那肽)的改进剂型被批准用于2型糖尿病患者
阿斯利康Bydureon(艾塞那肽)的改进剂型被批准用于2型糖尿病患者2017 年 10 月 23 日,阿斯利康已经宣布美国食品和药物管理局(FDA) 批准了Bydureon BCise(延长释放) 注射剂,这是新剂型Bydureon 的改进剂型,为每周一次,单次剂量自动注射,用于2 型糖尿病成人患者使用一个或多个口服药物且控制饮食和锻炼后仍无法控制血糖,帮助其改善血糖控制。
与其他类胰高血糖素多肽- 1(glp - 1) 受体激动剂不同的是,Bydureon BCise 有一个独特的、持续释放的微球传递系统,能够持续提供有效成分,帮助患者达到并保持稳定状态。
这个创新剂型的Bydureon BCise 装置被证明可以降低血糖水平,同时对减肥有帮助。
两项临床试验的数据显示,受试者使用Bydureon BCise 作为单一疗法,联用二甲双胍、磺酰脲类、噻唑烷二酮类三种口服降糖药之一或任意两种组合,持续服药28 周后平均糖化血红蛋白(HbA1c)减少 1.4%,平均体重减少 1.4 公斤。
在临床试验中超过5% 的患者报告的最常见的不良反应包括恶心(8.2%),以及注射部位结节不良反应 (10.5%)。
阿斯利康公司北美执行副总裁Dobber 表示:“我们了解到长期以来医生们已经对建立了对Bydureon 疗效的信心,因为Bydureon 能够显著降低HbA1c,为他们的病人提供了有效的治疗,帮助他们实现持续的血糖控制,还可以减肥。
Bydureon BCise 的批准让我们能够推出一个新的剂型,采用改进的易于使用的设备,这将有助于提高病人的体验。
”(2014年批准的Bydureon Pen是一种预填充的一次性笔式注射器)美国患者将在 2018 年第一季度获取到 Bydureon BCise。
目前欧洲药物管理局也接受了这个新的自动注射器装置的评审申请。
(来源:丁香园)。
艾塞那肽FDA说明书

HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use BYETTA safely and effectively. See full prescribing information for BYETTA.BYETTA® (exenatide) InjectionInitial U.S. Approval: 2005--------------------------RECENT MAJOR CHANGES------------------------Indications and Usage 10/2009Monotherapy and Combination Therapy (1.1)Important Limitations of Use 10/2009History of Pancreatitis (1.2)Warnings and Precautions 10/2009Pancreatitis (5.1)Renal Impairment (5.3)Macrovascular Outcomes (5.7)---------------------------INDICATIONS AND USAGE--------------------------- BYETTA is a glucagon-like peptide-1 (GLP-1) receptor agonist indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.Important Limitations of Use• BYETTA is not a substitute for insulin. BYETTA should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis(1.2).• The concurrent use of BYETTA with insulin has not been studied and cannot be recommended (1.2).• BYETTA has not been studied in patients with a history of pancreatitis.Consider other antidiabetic therapies in patients with a history ofpancreatitis (1.2).-------------------------DOSAGE AND ADMINISTRATION------------------- • Inject subcutaneously within 60 minutes prior to morning and evening meals (or before the two main meals of the day, approximately 6 hours or more apart) (2.1).• Initiate at 5 mcg per dose twice daily; increase to 10 mcg twice daily after 1 month based on clinical response (2.1).------------------------DOSAGE FORMS AND STRENGTHS------------------- BYETTA is supplied as 250 mcg/mL exenatide in:• 5 mcg per dose, 60 doses, 1.2 mL prefilled pen• 10 mcg per dose, 60 doses, 2.4 mL prefilled pen-----------------------------CONTRAINDICATIONS------------------------------ • History of severe hypersensitivity to exenatide or any product components(4.1).-----------------------WARNINGS AND PRECAUTIONS----------------------- • Pancreatitis: Postmarketing reports, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis. Discontinue BYETTA promptly.FULL PRESCRIBING INFORMATION: CONTENTS*1 INDICATIONS AND USAGE1.1 Type 2 Diabetes Mellitus1.2 Important Limitations of Use2 DOSAGE AND ADMINISTRATION2.1 Recommended Dosing3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS4.1 Hypersensitivity5 WARNINGS AND PRECAUTIONS5.1 Acute Pancreatitis5.2 Hypoglycemia5.3 Renal Impairment5.4 Gastrointestinal Disease5.5 Immunogenicity5.6 Hypersensitivity5.7 Macrovascular Outcomes6 ADVERSE REACTIONS6.1 Clinical Trial Experience6.2 Post-Marketing Experience7 DRUG INTERACTIONS7.1 Orally Administered Drugs7.2 Warfarin8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing MothersBYETTA should not be restarted. Consider other antidiabetic therapies in patients with a history of pancreatitis (5.1).• Hypoglycemia: Increased risk when BYETTA is used in combination witha sulfonylurea. Consider reducing the sulfonylurea dose (5.2).• Renal Impairment: Postmarketing reports, sometimes requiring hemodialysis and kidney transplantation. BYETTA should not be used in patients with severe renal impairment or end-stage renal disease and should be used with caution in patients with renal transplantation. Caution should be applied when initiating BYETTA or escalating the dose of BYETTA in patients with moderate renal failure (5.3).• Severe Gastrointestinal Disease: Use of BYETTA is not recommended in patients with severe gastrointestinal disease (e.g., gastroparesis) (5.4). • Hypersensitivity: Postmarketing reports of hypersensitivity reactions (e.g.anaphylaxis and angioedema). The patient should discontinue BYETTA and other suspect medications and promptly seek medical advice (5.6). • There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with BYETTA or any other antidiabetic drug(5.7).-----------------------------ADVERSE REACTIONS------------------------------- • Most common (≥5%) and occurring more frequently than placebo in clinical trials: nausea, hypoglycemia, vomiting, diarrhea, feeling jittery, dizziness, headache, dyspepsia. Nausea usually decreases over time (5.2;6).• Postmarketing reports of increased international normalized ratio (INR) with concomitant use of warfarin, sometimes with bleeding (6.2).To report SUSPECTED ADVERSE REACTIONS contact Amylin Pharmaceuticals, Inc. and Eli Lilly and Company at 1-800-868-1190 and or FDA at 1-800-FDA-1088 or /medwatch ------------------------------DRUG INTERACTIONS------------------------------ • Warfarin: Postmarketing reports of increased INR sometimes associated with bleeding. Monitor INR frequently until stable upon initiation oralteration of BYETTA therapy (7.2).-------------------------USE IN SPECIFIC POPULATIONS--------------------- • Pregnancy: Based on animal data, BYETTA may cause fetal harm.BYETTA should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. To report drug exposure duringpregnancy call 1-800-633-9081 (8.1).• Nursing Mothers: Caution should be exercised when BYETTA is administered to a nursing woman (8.3).See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.Revised: 10/20098.4 Pediatric Use8.5 Geriatric Use8.6 Renal Impairment8.7 Hepatic Impairment10 OVERDOSAGE11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment ofFertility13.3 Reproductive and Developmental Toxicology14 CLINICAL STUDIES14.1 Monotherapy14.2 Combination Therapy16 HOW SUPPLIED/STORAGE AND HANDLING16.1 How Supplied16.2 Storage and Handling17 PATIENT COUNSELING INFORMATION* Sections or subsections omitted from the full prescribing information are not listed.FULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGE1.1 Type 2 Diabetes MellitusBYETTA is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.1.2 Important Limitations of UseBYETTA is not a substitute for insulin. BYETTA should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis, as it would not be effective in these settings.The concurrent use of BYETTA with insulin has not been studied and cannot be recommended.Based on postmarketing data BYETTA has been associated with acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis. BYETTA has not been studied in patients with a history of pancreatitis. It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using BYETTA. Other antidiabetic therapies should be considered in patients with a history of pancreatitis.2 DOSAGE AND ADMINISTRATION2.1 Recommended DosingBYETTA should be initiated at 5 mcg administered twice daily at any time within the 60-minute period before the morning and evening meals (or before the two main meals of the day, approximately 6 hours or more apart). BYETTA should not be administered after a meal. Based on clinical response, the dose of BYETTA can be increased to 10 mcg twice daily after 1 month of therapy. Initiation with 5 mcg reduces the incidence and severity of gastrointestinal side effects. Each dose should be administered as a subcutaneous (SC) injection in the thigh, abdomen, or upper arm. No data are available on the safety or efficacy of intravenous or intramuscular injection of BYETTA.Use BYETTA only if it is clear, colorless and contains no particles.3 DOSAGE FORMS AND STRENGTHSBYETTA is supplied as a sterile solution for subcutaneous injection containing 250 mcg/mL exenatide in the following packages:• 5 mcg per dose, 60 doses, 1.2 mL prefilled pen• 10 mcg per dose, 60 doses, 2.4 mL prefilled peni p i a 4 CONTRAINDICATIONS4.1 HypersensitivityBYETTA is contraindicated in patients with prior severe hypersensitivity reactions to exenatide or to any of the product components.5 WARNINGS AND PRECAUTIONS5.1 Acute PancreatitisBased on postmarketing data BYETTA has been associated with acute pancreatitis,ncluding fatal and non-fatal hemorrhagic or necrotizing pancreatitis. After initiation ofBYETTA, and after dose increases, observe patients carefully for signs and symptoms ofancreatitis (including persistent severe abdominal pain, sometimes radiating to the back, which may or may not be accompanied by vomiting). If pancreatitis is suspected,BYETTA should promptly be discontinued and appropriate management should benitiated. If pancreatitis is confirmed, BYETTA should not be restarted. Considerntidiabetic therapies other than BYETTA in patients with a history of pancreatitis.5.2 HypoglycemiaThe risk of hypoglycemia is increased when BYETTA is used in combination with asulfonylurea (hypoglycemia can also occur when other antidiabetic agents are used incombination with a sulfonylurea). Therefore, patients receiving BYETTA and a sulfonylureamay require a lower dose of the sulfonylurea to reduce the risk of hypoglycemia. It is alsopossible that the use of BYETTA with other glucose-independent insulin secretagogues (e.g.meglitinides) could increase the risk of hypoglycemia.For additional information on glucose dependent effects see Mechanism of Action (12.1).5.3 Renal ImpairmentBYETTA should not be used in patients with severe renal impairment (creatinine clearance< 30 mL/min) or end-stage renal disease and should be used with caution in patients with renaltransplantation [see Use in Specific Populations (8.6)]. In patients with end-stage renal disease receiving dialysis, single doses of BYETTA 5 mcg were not well-tolerated due to gastrointestinal side effects. Because BYETTA may induce nausea and vomiting with transient hypovolemia,treatment may worsen renal function. Caution should be applied when initiating or escalatingdoses of BYETTA from 5 mcg to 10 mcg in patients with moderate renal impairment (creatinine clearance 30 to 50 mL/min).There have been postmarketing reports of altered renal function, including increased serumcreatinine, renal impairment, worsened chronic renal failure and acute renal failure, sometimesrequiring hemodialysis or kidney transplantation. Some of these events occurred in patientsreceiving one or more pharmacologic agents known to affect renal function or hydration status, such as angiotensin converting enzyme inhibitors, nonsteroidal anti-inflammatory drugs, or diuretics. Some events occurred in patients who had been experiencing nausea, vomiting, or diarrhea, with or without dehydration. Reversibility of altered renal function has been observed in many cases with supportive treatment and discontinuation of potentially causative agents, including BYETTA. Exenatide has not been found to be directly nephrotoxic in preclinical or clinical studies.5.4 Gastrointestinal DiseaseBYETTA has not been studied in patients with severe gastrointestinal disease, including gastroparesis. Because BYETTA is commonly associated with gastrointestinal adverse reactions, including nausea, vomiting, and diarrhea, the use of BYETTA is not recommended in patients with severe gastrointestinal disease.5.5 ImmunogenicityPatients may develop antibodies to exenatide following treatment with BYETTA, consistent with the potentially immunogenic properties of protein and peptide pharmaceuticals. In a small proportion of patients, the formation of antibodies to exenatide at high titers could result in failure to achieve adequate improvement in glycemic control. If there is worsening glycemic control or failure to achieve targeted glycemic control, alternative antidiabetic therapy should be considered [see Adverse Reactions (6.1)].5.6 HypersensitivityThere have been postmarketing reports of serious hypersensitivity reactions (e.g. anaphylaxis and angioedema) in patients treated with BYETTA. If a hypersensitivity reaction occurs, the patient should discontinue BYETTA and other suspect medications and promptly seek medical advice [see Adverse Reactions (6.2)].5.7 Macrovascular OutcomesThere have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with BYETTA or any other antidiabetic drug.6 ADVERSE REACTIONS6.1 Clinical Trial ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.HypoglycemiaTable 1 summarizes the incidence and rate of hypoglycemia with BYETTA in five placebo-controlled clinical trials.Table 1: Incidence (%) and Rate of Hypoglycemia When BYETTA was Used as Monotherapy or WithConcomitant Antidiabetic Therapy in Five Placebo-Controlled Clinical Trials*BYETTAPlacebo twice daily 5 mcg twice daily 10 mcg twice dailyMonotherapy (24 Weeks)77 77 78N%1.3% 5.2% 3.8%OverallRate0.03 0.21 0.52 (episodes/patientyear)% Severe 0.0% 0.0% 0.0%With Metformin (30 Weeks)N 113 110 1135.3% 4.5% 5.3%Overall%Rate0.12 0.13 0.12 (episodes/patientyear)% Severe 0.0% 0.0% 0.0%With a Sulfonylurea (30 Weeks)N 123 125 129 % Overall 3.3% 14.4% 35.7%Rate0.07 0.64 1.61 (episodes/patientyear)% Severe 0.0% 0.0% 0.0%With Metformin and a Sulfonylurea (30 Weeks)N 247 245 241 % Overall 12.6% 19.2% 27.8%Rate0.58 0.78 1.71 (episodes/patientyear)% Severe 0.0% 0.4% 0.0%With a Thiazolidinedione (16 Weeks)N 112 Dose not studied 121% Overall 7.1% Dose not studied 10.7%Rate0.56 Dose not studied 0.98(episodes/patientyears)% Severe 0.0% Dose not studied 0.0%* For the 30-week trials, a hypoglycemia episode was recorded if the patient reported symptoms consistent with hypoglycemia and was recorded as severe if the subject required the assistance of another person to treat theevent. For the other trials, a hypoglycemic episode was recorded if a patient reported signs or symptoms ofhypoglycemia or had a blood glucose value consistent with hypoglycemia regardless of associated symptoms ortreatment and was recorded as severe if the subject required the assistance of another person to treat the event.The requirement for assistance had to be accompanied by a blood glucose measurement of <50 mg/dL orprompt recovery after administration of oral carbohydrate.N = The number of Intent-to-Treat subjects in each treatment group.Immunogenicitypatients had low titer antibodies to exenatide at 30 weeks. For this group, the level of glycemic control (hemoglobin A1c [HbA1c]) was generally comparable to that observed in those without antibody titers. An additional 6% of patients had higher titer antibodies at 30 weeks. In about half of this 6% (3% of the total patients given BYETTA in the 30-week controlled studies), the glycemic response to BYETTA was attenuated; the remainder had a glycemic response comparable to that of patients without antibodies.In the 16-week trial of BYETTA add-on to thiazolidinediones, with or without metformin, 9% of patients had higher titer antibodies at 16 weeks. In the 24-week trial of BYETTA used as monotherapy, 3% of patients had higher titer antibodies at 24 weeks. Compared with patients who did not develop antibodies to BYETTA, on average the glycemic response in patients with higher titer antibodies was attenuated [see Warnings and Precautions (5.5)].Other Adverse ReactionsMonotherapyFor the 24-week placebo-controlled study of BYETTA used as a monotherapy, Table 2 summarizes adverse reactions (excluding hypoglycemia) occurring with an incidence ≥2% and occurring more frequently in BYETTA-treated patients compared with placebo-treated patients. Table 2: Treatment-Emergent Adverse Reactions ≥2% Incidence With BYETTA Used as Monotherapy (Excluding Hypoglycemia)*Monotherapy Placebo BIDN = 77%All BYETTA BIDN = 155%Nausea 0 8Vomiting 0 4Dyspepsia 0 3 * In a 24-week placebo-controlled trial.BID = twice daily.Adverse reactions reported in ≥1.0 to <2.0% of patients receiving BYETTA and reported more frequently than with placebo included decreased appetite, diarrhea, and dizziness. The most frequently reported adverse reaction associated with BYETTA, nausea, occurred in a dose-dependent fashion.Two of the 155 patients treated with BYETTA withdrew due to adverse reactions of headache and nausea. No placebo-treated patients withdrew due to adverse reactions.Combination TherapyAdd-on to metformin and/or sulfonylureaadverse reactions (excluding hypoglycemia) with an incidence ≥2% and occurring more frequently in BYETTA-treated patients compared with placebo-treated patients [see Warnings and Precautions (5.2)] are summarized in Table 3.Table 3: Treatment-Emergent Adverse Reactions ≥2% Incidence and Greater Incidence With BYETTA Treatment Used With Metformin and/or a Sulfonylurea (Excluding Hypoglycemia)*Placebo BID N = 483% All BYETTA BIDN = 963%Nausea 18 44Vomiting 4 13Diarrhea 6 13 Feeling Jittery 4 9Dizziness 6 9Headache 6 9Dyspepsia 3 6Asthenia 2 4 Gastroesophageal RefluxDisease1 3Hyperhidrosis 1 3 * In three 30-week placebo-controlled clinical trials.BID = twice daily.Adverse reactions reported in ≥1.0 to <2.0% of patients receiving BYETTA and reported morefrequently than with placebo included decreased appetite. Nausea was the most frequentlyreported adverse reaction and occurred in a dose-dependent fashion. With continued therapy, the frequency and severity decreased over time in most of the patients who initially experiencednausea. Patients in the long-term uncontrolled open-label extension studies at 52 weeks reportedno new types of adverse reactions than those observed in the 30-week controlled trials.The most common adverse reactions leading to withdrawal for BYETTA-treated patients werenausea (3% of patients) and vomiting (1%). For placebo-treated patients, <1% withdrew due tonausea and none due to vomiting.Add-on to thiazolidinedione with or without metforminFor the 16-week placebo-controlled study of BYETTA add-on to a thiazolidinedione, with orwithout metformin, Table 4 summarizes the adverse reactions (excluding hypoglycemia) with an incidence of ≥2% and occurring more frequently in BYETTA-treated patients compared withplacebo-treated patients.Table 4: Treatment-Emergent Adverse Reactions ≥2% Incidence With BYETTA Used With a Thiazolidinedione, With or Without Metformin (Excluding Hypoglycemia)*With a TZD or TZD/MET PlaceboN = 112%All BYETTA BIDN = 121%Nausea 15 40Vomiting 1 13Dyspepsia 1 7Diarrhea 3 6 GastroesophagealReflux Disease0 3* In a 16-week placebo-controlled clinical trial.BID = twice daily.Adverse reactions reported in ≥1.0 to <2.0% of patients receiving BYETTA and reported more frequently than with placebo included decreased appetite. Chills (n = 4) and injection-sitereactions (n = 2) occurred only in BYETTA-treated patients. The two patients who reported an injection-site reaction had high titers of antibodies to exenatide. Two serious adverse events(chest pain and chronic hypersensitivity pneumonitis) were reported in the BYETTA arm. Noserious adverse events were reported in the placebo arm.The most common adverse reactions leading to withdrawal for BYETTA-treated patients werenausea (9%) and vomiting (5%). For placebo-treated patients, <1% withdrew due to nausea.6.2 Post-Marketing ExperienceThe following additional adverse reactions have been reported during post-approval use of BYETTA. Because these events are reported voluntarily from a population of uncertain size, itis generally not possible to reliably estimate their frequency or establish a causal relationship todrug exposure.Allergy/Hypersensitivity: injection-site reactions, generalized pruritus and/or urticaria, macularor papular rash, angioedema, anaphylactic reaction [see Warnings and Precautions (5.6)].Drug Interactions: International normalized ratio (INR) increased with concomitant warfarin use sometimes associated with bleeding [see Drug Interactions (7.2)].Gastrointestinal: nausea, vomiting, and/or diarrhea resulting in dehydration; abdominaldistension, abdominal pain, eructation, constipation, flatulence, acute pancreatitis, hemorrhagicand necrotizing pancreatitis sometimes resulting in death [see Limitations of Use (1.2) andWarnings and Precautions (5.1)].Neurologic: dysgeusia; somnolenceRenal and Urinary Disorders: altered renal function, including increased serum creatinine, renal impairment, worsened chronic renal failure or acute renal failure (sometimes requiringhemodialysis), kidney transplant and kidney transplant dysfunction [see Warnings and Precautions (5.3)].7 DRUG INTERACTIONS7.1 Orally Administered DrugsThe effect of BYETTA to slow gastric emptying can reduce the extent and rate of absorption of orally administered drugs. BYETTA should be used with caution in patients receiving oral medications that have narrow therapeutic index or require rapid gastrointestinal absorption [see Adverse Reactions (6.2)]. For oral medications that are dependent on threshold concentrations for efficacy, such as contraceptives and antibiotics, patients should be advised to take those drugs at least 1 hour before BYETTA injection. If such drugs are to be administered with food, patients should be advised to take them with a meal or snack when BYETTA is not administered [see Clinical Pharmacology (12.3)].7.2 WarfarinThere are postmarketing reports of increased INR sometimes associated with bleeding, with concomitant use of warfarin and BYETTA [see Adverse Reactions (6.2)]. In a drug interaction study, BYETTA did not have a significant effect on INR [see Clinical Pharmacology (12.3)]. In patients taking warfarin, prothrombin time should be monitored more frequently after initiation or alteration of BYETTA therapy. Once a stable prothrombin time has been documented, prothrombin times can be monitored at the intervals usually recommended for patients on warfarin.8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category CThere are no adequate and well-controlled studies of BYETTA use in pregnant women. In animal studies, exenatide caused cleft palate, irregular skeletal ossification and an increased number of neonatal deaths. BYETTA should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.Female mice given SC doses of 6, 68, or 760 mcg/kg/day beginning 2 weeks prior to and throughout mating until gestation day 7 had no adverse fetal effects. At the maximal dose,760 mcg/kg/day, systemic exposures were up to 390 times the human exposure resulting from the maximum recommended dose of 20 mcg/day, based on AUC [see Nonclinical Toxicology (13.3)].In developmental toxicity studies, pregnant animals received exenatide subcutaneously during organogenesis. Specifically, fetuses from pregnant rabbits given SC doses of 0.2, 2, 22, 156, or260 mcg/kg/day from gestation day 6 through 18 experienced irregular skeletal ossifications from exposures 12 times the human exposure resulting from the maximum recommended dose of 20 mcg/day, based on AUC. Moreover, fetuses from pregnant mice given SC doses of 6, 68, 460, or 760 mcg/kg/day from gestation day 6 through 15 demonstrated reduced fetal and neonatal growth, cleft palate and skeletal effects at systemic exposure 3 times the human exposure resulting from the maximum recommended dose of 20 mcg/day, based on AUC [see Nonclinical Toxicology (13.3)].Lactating mice given SC doses of 6, 68, or 760 mcg/kg/day from gestation day 6 through lactation day 20 (weaning), experienced an increased number of neonatal deaths. Deaths were observed on postpartum days 2-4 in dams given 6 mcg/kg/day, a systemic exposure 3 times the human exposure resulting from the maximum recommended dose of 20 mcg/day, based on AUC [see Nonclinical Toxicology (13.3)].Pregnancy RegistryAmylin Pharmaceuticals, Inc. maintains a Pregnancy Registry to monitor pregnancy outcomes of women exposed to exenatide during pregnancy. Physicians are encouraged to register patients by calling 1-800-633-9081.8.3 Nursing MothersIt is not known whether exenatide is excreted in human milk. However, exenatide is present at low concentrations (less than or equal to 2.5% of the concentration in maternal plasma following subcutaneous dosing) in the milk of lactating mice. Many drugs are excreted in human milk and because of the potential for clinically significant adverse reactions in nursing infants from exenatide, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account these potential risks against the glycemic benefits to the lactating woman. Caution should be exercised when BYETTA is administered to a nursing woman.8.4 Pediatric UseSafety and effectiveness of BYETTA have not been established in pediatric patients.8.5 Geriatric UsePopulation pharmacokinetic analysis of patients ranging from 22 to 73 years of age suggests that age does not influence the pharmacokinetic properties of exenatide [see Clinical Pharmacology (12.3)]. BYETTA was studied in 282 patients 65 years of age or older and in 16 patients75 years of age or older. No differences in safety or effectiveness were observed between these patients and younger patients. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection in the elderly based on renal function.8.6 Renal ImpairmentBYETTA is not recommended for use in patients with end-stage renal disease or severe renal impairment (creatinine clearance < 30 mL/min) and should be used with caution in patients with renal transplantation. No dosage adjustment of BYETTA is required in patients with mild renal impairment (creatinine clearance 50 to 80 mL/min). Caution should be applied when initiating or escalating doses of BYETTA from 5 mcg to 10 mcg in patients with moderate renal impairment (creatinine clearance 30 to 50 mL/min) [see Clinical Pharmacology (12.3)].8.7 Hepatic ImpairmentNo pharmacokinetic study has been performed in patients with a diagnosis of acute or chronic hepatic impairment. Because exenatide is cleared primarily by the kidney, hepatic dysfunction is not expected to affect blood concentrations of exenatide [see Clinical Pharmacology (12.3)].10 OVERDOSAGEIn a clinical study of BYETTA, three patients with type 2 diabetes each experienced a single overdose of 100 mcg SC (10 times the maximum recommended dose). Effects of the overdoses included severe nausea, severe vomiting, and rapidly declining blood glucose concentrations. One of the three patients experienced severe hypoglycemia requiring parenteral glucose administration. The three patients recovered without complication. In the event of overdose, appropriate supportive treatment should be initiated according to the patient’s clinical signs and symptoms.11 DESCRIPTIONBYETTA (exenatide) is a synthetic peptide that was originally identified in the lizard Heloderma suspectum. Exenatide differs in chemical structure and pharmacological action from insulin, sulfonylureas (including D-phenylalanine derivatives and meglitinides), biguanides, thiazolidinediones, alpha-glucosidase inhibitors, amylinomimetics and dipeptidyl peptidase-4 inhibitors.Exenatide is a 39-amino acid peptide amide. Exenatide has the empirical formulaC184H282N50O60S and molecular weight of 4186.6 Daltons. The amino acid sequence for exenatide is shown below.H-His-Gly-Glu-Gly-Thr-Phe-Thr-Ser-Asp-Leu-Ser-Lys-Gln-Met-Glu-Glu-Glu-Ala-Val-Arg-Leu -Phe-Ile-Glu-Trp-Leu-Lys-Asn-Gly-Gly-Pro-Ser-Ser-Gly-Ala-Pro-Pro-Pro-Ser-NH2BYETTA is supplied for SC injection as a sterile, preserved isotonic solution in a glass cartridge that has been assembled in a pen-injector (pen). Each milliliter (mL) contains 250 micrograms (mcg) synthetic exenatide, 2.2 mg metacresol as an antimicrobial preservative, mannitol as a tonicity-adjusting agent, and glacial acetic acid and sodium acetate trihydrate in water for。
艾塞那肽缓释制剂说明书

百达扬说明书
百达扬说明书 Prepared on 22 November 2020【药品名称】商品名称:百达扬通用名称:注射用艾塞那肽微球英文名称:Exenatide Microspheres for Injection【成份】注射用艾塞那肽微球活性成份为艾塞那肽。
辅料:注射用艾塞那肽微球:乙交酯丙交酯共聚物(50:50),蔗糖。
注射用溶剂:羧甲基纤维素钠、氯化钠、聚山梨酯20、磷酸二氢钠一水合物、磷酸氢二钠七水合物、注射用水。
【适应症】用于改善患者的血糖控制,适用于单用二甲双胍、磺脲类以及二甲双胍合用磺脲类血糖仍控制不佳的患者。
【用法用量】推荐用量注射用艾塞那肽微球(2mg)应每7天(每周)皮下注射一次。
可在一天中的任何时间注射,空腹或进食后均可。
漏用如漏用一次且距离下次预定用药至少3天以上,应在发现后尽快注射。
此后,患者可恢复其每7天(每周)一次的常规用药计划。
如漏用一次且距离下次预定用药1或2天,患者不应给予漏掉剂量而应在下次预定用药时按照常规计划注射。
改变每周用药方案如果有需要可改变每周的用药日,只要与上次注射至少间隔3天。
用法注射用艾塞那肽微球由患者自行给药,需要混合药物和填充注射器。
一旦将药物混合后,必须立即注射。
用药应在腹部、大腿或上臂区域皮下(SC)注射。
告知患者在同一区域注射时,每周选择不同的部位。
禁止静脉注射或肌肉注射。
给药前,患者应接受医疗专业人员的培训。
完整的用药说明(带图示)请参见注射用艾塞那肽微球的使用手册。
【不良反应】肾功能损害重度肾功能损害(肌酐清除率<30mL/min)或终末期肾病患者不应使用注射用艾塞那肽微球,在肾移植患者中应谨慎使用。
接受透析的终末期肾病患者,由于发生胃肠道不良反应,不能很好地耐受单剂量5μg塞那肽注射液。
由于注射用艾塞那肽微球可能引起恶心、呕吐伴一过性低血容量,故治疗可能造成肾功能损害加重。
中度肾功能损害患者(肌酐清除率30至50mL/min)使用注射用艾塞那肽微球时应谨慎。
艾塞那肽概况
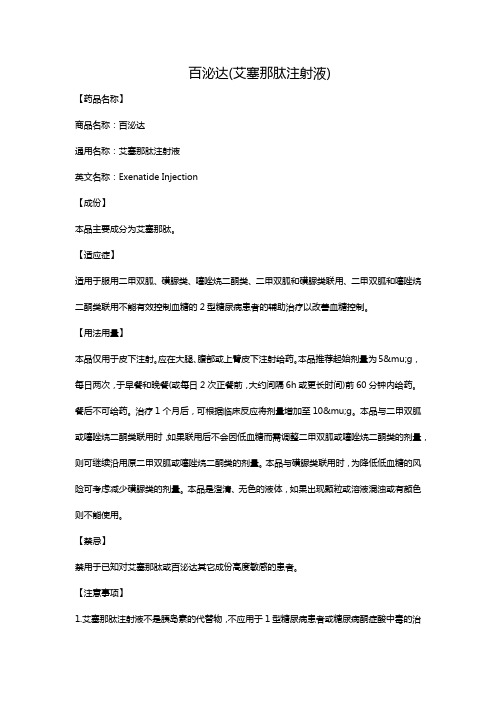
醋酸艾塞那肽项目介绍一)艾塞那肽(Exendin-4)介绍:艾塞那肽是从墨西哥巨蜥蜴毒液中分离出来的一种含有39个氨基酸的多肽序列,与GLP-1(胰高血糖素样肽,氨基酸序列:HDEFERHAEGTFTSDVSSYLEGQAAKEFIAWLVKTRG-OH)具有53%的同源性。
可促进胰岛素分泌,具有半衰期长的优点,主要应用在Ⅱ型糖尿病治疗方面。
商品名为百泌达(Bydureon),2011年欧盟获批,2012年FDA批准上市。
艾塞那肽序列:单字母表示:HGEGTFTSDL SKQMEEEAVR LFIEWLKNGG PSSGAPPPS –NH2三字母表示:H-His - Gly - Glu - Gly - Thr - Phe - Thr - Ser - Asp - Leu - Ser - Lys - Gln - Met - Glu - Glu - Glu - Ala - Val - Arg - Leu - Phe - Ile - Glu - Trp - Leu - Lys - Asn - Gly - Gly - Pro - Ser - Ser - Gly - Ala - Pro - Pro - Pro - Ser –NH2分子式:C184H282N50O60S1CAS NO:141758-74-9残基数:39分子量:4186.63 g/mol等电点:pH 4.86溶解性预测:较好的水溶性图1 艾塞那肽亲水性分析注:1)上边是亲水性,下边是疏水性2)颜色表示: Acidic酸性Aromatic芳香性Basic碱性Aliphatic脂肪族Polar极性Cysteine半胱氨酸二)醋酸艾塞那肽(exenatide acetate)分子式:C184H282N50O60S.C2H4O2分子量:4262.67CAS NO:141732-76-5三)艾塞那肽合成:合成方法:固相合成合成树脂:Rink Amide MBHA Resin(loading: 0.3mmol/g)溶剂:DMF脱保护试剂:20% PIP切割试剂:TFA/ED T/ Thioanisole / 2-Mercaptoethanol图2 艾塞那肽合成流程图四)HPLC 纯化(TFA盐艾塞那肽)1)色谱填料选择。
百泌达(艾塞那肽注射液)
百泌达(艾塞那肽注射液)【药品名称】商品名称:百泌达通用名称:艾塞那肽注射液英文名称:Exenatide Injection【成份】本品主要成分为艾塞那肽。
【适应症】适用于服用二甲双胍、磺脲类、噻唑烷二酮类、二甲双胍和磺脲类联用、二甲双胍和噻唑烷二酮类联用不能有效控制血糖的2型糖尿病患者的辅助治疗以改善血糖控制。
【用法用量】本品仅用于皮下注射。
应在大腿、腹部或上臂皮下注射给药。
本品推荐起始剂量为5μg,每日两次,于早餐和晚餐(或每日2次正餐前,大约间隔6h或更长时间)前60分钟内给药。
餐后不可给药。
治疗1个月后,可根据临床反应将剂量增加至10μg。
本品与二甲双胍或噻唑烷二酮类联用时,如果联用后不会因低血糖而需调整二甲双胍或噻唑烷二酮类的剂量,则可继续沿用原二甲双胍或噻唑烷二酮类的剂量。
本品与磺脲类联用时,为降低低血糖的风险可考虑减少磺脲类的剂量。
本品是澄清、无色的液体,如果出现颗粒或溶液混浊或有颜色则不能使用。
【禁忌】禁用于已知对艾塞那肽或百泌达其它成份高度敏感的患者。
【注意事项】1.艾塞那肽注射液不是胰岛素的代替物,不应用于1型糖尿病患者或糖尿病酮症酸中毒的治疗。
2.有使用艾塞那肽注射液治疗的患者发生急性胰腺炎个案报道。
应告知患者伴有呕吐的持续性、严重腹痛是急性胰腺炎的标志性症状。
如果怀疑发生急性胰腺炎,应停用艾塞那肽注射液和其他可疑药物,并进行确证试验和适当治疗。
如果证实是胰腺炎,但病因不明时,不推荐继续用艾塞那肽注射液治疗。
3.给与艾塞那肽注射液治疗后患者可能会产生抗艾塞那肽抗体,这与蛋白质和肽类药物的潜在免疫原性特点有关。
接受艾塞那肽注射液治疗的患者应注意观察是否有发生过敏性反应的症状和体征。
少部分患者由于产生的抗艾塞那肽抗体效价高可能会导致不能改善血糖控制。
如果血糖控制情况恶化或不能达到血糖控制目标,应考虑选择其他抗糖尿病疗法。
4.尚未进行艾塞那肽注射液与胰岛素、D-苯丙氨酸衍生物、氯茴苯酸类或α-葡萄糖苷酶抑制剂联用的研究。
艾塞那肽 Bydureon
艾塞那肽注射液缓释制剂Bydureon一、项目基本信息CAS number: 141758-74-9上市情况:2011年6月在欧盟获批2012年1月27日获得FDA批准上市适应症:与二甲双胍、磺脲类药物和噻唑烷二酮等单药或多药联合使用治疗2型糖尿病。
剂型与规格:2mg,粉剂和注射用缓释混悬剂。
背景Bydureon(艾塞那肽注射液缓释剂型)是Amylin和礼来糖尿病药物Byetta(百泌达,艾塞那肽注射液)的长效版本,该控释剂型是利用Alkermes 公司专有技术在一周的时间里控制艾塞那肽的释放。
Bydureon只需每周注射使用一次来控制2型糖尿病患者的血糖,而百泌达则需要每天注射2次。
百泌达作为第一个也是唯一被SFDA批准上市的GLP-1受体激动剂,具有人体GLP-1的相似的作用机理和益处,可以增强葡萄糖依赖性胰岛素分泌,并显示出抗高血糖作用。
百泌达需要1天两次皮下注射,分别在早餐和晚餐前1小时内注射。
它的使用方法很简单,通过一个简便易用的笔型装置就可以注射。
但是它的剂量与胰岛素不同,每一次给药剂量都是固定的,不需要根据血糖水平而随时作调整。
百泌达的独特优势在临床和实际使用中已经被证明,其中包括:改善β细胞的功能;长期有效控制血糖,疗效卓越;葡萄糖依赖性的调控血糖,低血糖风险低;可降低患者体重;固定剂量,使用简单。
临床试验在长期试验中,Bydureon相对Byetta全面进行了24周的测试。
结果显示,使用Bydureon的患者改善了血糖控制,糖化血红蛋白指标与基线相比下降1.5%-1.9%,相比之下,使用Byetta 的患者只有0.9%。
此外,与使用Byetta具有相同的减轻体重作用。
主要的临床副反应是轻中度的恶心(与使用Byetta 的患者(35%)相比,使用Bydureon的患者(14%)更少出现该反应。
)、呕吐和腹泻,上呼吸道感染和注射部位结节,没有严重的低血糖事件。
中国目前约有2400万糖尿病患者,至2025年预计将达4613万。
艾塞那肽注射液说明书

核准日期:年月日艾塞那肽注射液说明书请仔细阅读说明书并在医师指导下使用对艾塞那肽及其它成份过敏者禁用【药物名称】通用名称:艾塞那肽注射液英文名称:Exenatide Injection汉语拼音:Aisainatai Zhusheye【成份】本品主要成份为艾塞那肽。
化学结构式:分子式:C184H282N50O60S分子量:4186.6辅料:甘露醇、醋酸钠三水合物、间甲酚(2.00-2.4mg/ml)、冰醋酸、注射用水。
【性状】本品为无色澄明液体【适应症】本品用于改善2型糖尿病患者的血糖控制,适用于单用二甲双胍、磺酰脲类,以及二甲双胍合用磺酰脲类,血糖仍控制不佳的患者。
【规格】(1)5μg剂量刻度注射笔:0.25 mg/ml,1.2 ml/支,单次注射药量5μg,内含60次注射的药量。
(2)10μg剂量刻度注射笔:0.25 mg/ml,2.4 ml/支,单次注射药量10μg,内含60次注射的药量。
【用法用量】本品的起始剂量为每次5微克(μg),每日2次,在早餐和晚餐前60分钟内(或每天的2顿主餐前;给药间隔大约6小时或更长)皮下注射。
不应在餐后注射本品。
根据临床应答,在治疗1个月后剂量可增加至10微克。
每日2次。
每次给药应在大腿、腹部或上臂皮下注射给药。
本品推荐用于接受二甲双胍、一种磺酰脲类、二甲双胍合用一种磺酰脲类治疗,血糖仍控制不佳的2型糖尿病患者。
在二甲双胍治疗的基础上加用本品时,可继续使用二甲双胍的目前剂量,因为合用本品发生低血糖而需要进行调整二甲双胍剂量的可能性较低。
在磺酰脲类治疗基础上加用本品,应该考虑降低磺酰脲类的剂量,以降低低血糖发生的风险。
(参照【注意事项】,低血糖)本品为无色澄明液体,当溶液有颗粒、浑浊或变色时不得使用。
过有效期后不得使用。
尚无本品静脉或肌肉注射的安全性和有效性资料。
注射笔使用指南注射笔的详细操作图示和注射指导请参见本品包装盒中所附“注射笔使用手册”。
重要提示使用本注射笔前请仔细阅读“注射笔使用手册”,如果不完全按照使用手册操作可能会出现剂量错误、注射笔损坏或者发生感染。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
【药物名称】
中文通用名称:艾塞那肽
英文通用名称:Exenatide
其他名称:Byetta。
【临床应用】
作为辅助用药,用于单服二甲双胍或磺酰脲类药或联用二甲双胍和磺酰脲类药后均未达到充分血糖控制的2型糖尿病患者的血糖控制的改善。
(国外资料)
【药理】
1.药效学本药是一种合成的肠降血糖素类似物(有抗高血糖作用的肽),其53%的氨基酸顺序与哺乳动物胰高血糖素样多肽-1(GLP-1)的氨基酸顺序相同,但不是GLP-1的类似物。
GLP-1是一种肠道激素,是肠道L细胞响应营养摄入而分泌的激素,可通过其受体产生降血糖和抗糖尿病作用(如刺激葡萄糖依赖性胰岛素的释放,抑制胰高血糖素的分泌),但半衰期较短[低于2分钟,主要经蛋白水解酶Ⅳ(二肽酰胺酶Ⅳ)快速降解]。
本药可激动GLP-1受体,产生与GLP-1类似的作用[其许多(或所有)抗糖尿病作用似与GLP-1受体结合有关,但观察到的所有药效学作用与GLP-1的作用并不一致,有研究人员认为,这可能是本药通过功能不同的其他受体而产生的]。
其作用包括:增强葡萄糖依赖性的胰岛素的分泌和抑制葡萄糖依赖性的异常增高的胰高血糖素的分泌、减慢胃排空、减少食物摄入、促进β-细胞增殖和再生、减少脂肪堆积及胰岛素增敏作用(动物模型)。
由于本药相对较能抵抗蛋白水解酶Ⅳ(二肽酰胺酶Ⅳ)的降解(因GLP-1的2位存在一个丙氨酸基团,可被蛋白水解酶Ⅳ识别,而本药2位则为甘氨酸基团),故有较长的半衰期,体内活性较GLP-1增强。
一项安慰剂对照研究提示,本药可显著降低禁食状态的血浆葡萄糖水平,降低餐后葡萄糖相对于基础值的峰变化;用药后观察到胃排空延迟、热量摄入减少。
资料表明,本药在非糖尿病受试者及2型糖尿病患者中均是一种强效促胰岛素分泌药。
2.药动学予2型糖尿病患者皮下注射本药,可见餐后葡萄糖水平降低持续达5小时,注射后约3小时达最低点。
2型糖尿病患者皮下注射10μg后2.1小时)211pg/ml,曲线下面积(AUC)为1.036(ng·h)/ml。
动物研究中,达峰浓度(C
max
经皮下注射给药的生物利用度为65%-75%,尚无人类的生物利用度资料。
皮下注射和静脉给药的分布容积分别为28.3L(与剂量、年龄、性别、种族和患者的体型无关)和64ml/kg(健康受试者)。
药物在人体内的代谢尚不明确,但动物研究表明本药较GLP-1更能抵抗蛋白水解酶Ⅳ的降解。
本药主要经肾小球过滤清除,随后经蛋白水解降解,平均肾清除率为9.1L/h,终末半衰期为2.4小时,轻至中度肾损害者(肌酐清除率30-80ml/min)的平均肾清除率减至0.9L/h。
肾清除率和半衰期均与剂量、年龄、性别、种族和患者的体型无关。
3.遗传与生殖毒性动物研究表明本药对胎仔有不良效应(致畸、致死胎或其他)。
1.特别警示本药可能导致胰腺炎。
2.禁忌症(1)对本药过敏者。
(2)1型糖尿病患者。
(3)糖尿病性酮症酸中毒患者。
(4)晚期肾疾病或严重肾损害(肌酐清除率低于30ml/min)患者不推荐使用本药。
(5)严重胃肠道疾病(如胃轻瘫)患者不推荐使用本药。
(以上均选自国外资料)
3.慎用低血糖者(与磺酰脲类同用则风险增加)(国外资料)。
4.药物对儿童的影响儿童用药的安全性和疗效尚未确立。
5.药物对妊娠的影响尚无孕妇用药的安全性数据,孕妇用药应权衡利弊。
美国食品药品管理局(FDA)对本药的妊娠安全性分级为C级。
6.药物对哺乳的影响本药可分泌入哺乳小鼠的乳汁中,尚无哺乳妇女用药的安全性数据,哺乳期用药应权衡利弊。
【不良反应】
[国外不良反应参考]
1.心血管系统未见对心率、血压或ECG等参数的影响。
2.代谢/内分泌系统(1)可见低血糖(5%-36%)。
和联用磺酰脲类后出现轻至中度低血糖,且呈剂量依赖性,口服碳水化合物后症状消除。
和联用二甲双胍时罕见低血糖发生。
(2)据报道,本药治疗第1日,皮质醇水平轻度升高,第28日后恢复正常。
3.免疫系统有资料显示,可见本药抗体产生,但似乎对降低糖基化血红蛋白水平无影响。
4.神经可见头晕(9%)、头痛(9%)、神经质(9%)。
5.胃肠道可见腹泻(13%)、消化不良(6%)、恶心(44%)、呕吐(13%)。
此外,本药可能导致胰腺炎。
【药物相互作用】
·药物-药物相互作用
1.与对乙酰氨基酚合用,可致对乙酰氨基酚的AUC、峰浓度及生物利用度降低,达峰时间延长。
其机制可能与胃排空减慢引起对乙酰氨基酚吸收减少有关。
两药联用时,应至少在使用本药前1小时给予对乙酰氨基酚。
2.与洛伐他汀合用,可致洛伐他汀的AUC、峰浓度及生物利用度降低。
其机制可能与胃排空减慢引起洛伐他汀吸收减少有关。
合用时可能需增加洛伐他汀剂量以弥补其生物利用度的降低,并有必要监测血脂。
【给药说明】
1.对需用胰岛素的患者,本药不能取代胰岛素。
2.使用胰岛素、噻唑烷二酮、右旋苯丙氨衍生物、瑞格列奈类或α-葡萄糖苷酶抑制药的患者应慎用本药。
3.用药后若怀疑出现胰腺炎,应停药。
若确诊胰腺炎由本药引起,应永久性停用本药。
[国外用法用量参考]
成人
·常规剂量
·皮下注射初始剂量,一次5μg,一日2次;维持剂量,一次10μg,一日2次。
·肾功能不全时剂量
不推荐晚期肾脏疾病或严重肾损害者(肌酐清除率低于30ml/min)使用本药。
【制剂与规格】
艾塞那肽注射液1ml:250μg。
贮法:2-8℃冷藏、避光保存,严禁冷冻。