坎格列净片OFFICE DIRECTOR MEMO
【卡格列净片是什么?】

【卡格列净⽚是什么?】⽂章导读卡格列净⽚是⼀种⽐较常见的药物,这种药物主要是可以有效治疗⼈体糖尿病等,可以起到降⾎糖等功效,⽽糖尿病是⼈体⽐较常见的⼀种慢性疾病,患有⾼⾎糖不仅会容易影响到⾝体健康,同时也会容易导致⼀些并发症等,可以服⽤卡格列净⽚来进⾏治疗。
卡格列净⽚是什么?卡格列净是适⽤于糖尿病病⼈的⼀种降糖药,它属于SGLT2抑制剂类降糖药物,这类降糖药物是⽬前⽐较新型的降糖药物。
糖尿病是⼀种以⾎糖升⾼为表现的疾病,卡格列净可以增加⼩便中葡萄糖的排除,⾎中的葡萄糖被更多的排除体外后,⾎糖就会降低,这就是卡格列净具有降糖作⽤的原因。
在使⽤过程中,由于尿中的糖增加了,所以这个时候测尿糖就会升⾼,这是药物起效的表现。
怡可安与⼆甲双胍联⽤:当单独使⽤⼆甲双胍⾎糖控制不佳时,可与⼆甲双胍联合使⽤,配合饮⾷和运动成⼈2型糖尿病患者的⾎糖控制。
怡可安与⼆甲双胍和磺脲类药物联⽤:当联⽤⼆甲双胍和磺脲类药物⾎糖控制不佳时,可与⼆甲双胍和磺脲类药物联合使⽤,配合饮⾷和运动成⼈2型糖尿病患者的⾎控制。
怡可安主要成分是卡格列净,卡格列净是⼀种钠-葡萄糖协调转运蛋⽩(SGLT2)抑制剂,肾⼩管管腔滤过的葡萄糖主要经表达于近端肾⼩管的SGLT2进⾏重吸收,卡格列净通过抑制SGLT2减少肾脏对滤过葡萄糖的重吸收,降低肾糖阈,增加尿糖排泄,从⽽降低⾎糖。
糖尿病是常见的慢性病之⼀,患上糖尿病的⼈很多,不同病⼈⽤药选择不同,患者需要根据实际的患病情况选择对症的药物进⾏使⽤,⽤药之前也需要了解清楚相关的药物信息,那么下⾯我们⼀起来看看怡可安相应的药理作⽤是什么?怡可安药理作⽤:卡格列净是⼀种钠-葡萄糖协同转运蛋⽩(SGLT2)抑制剂。
肾⼩管管腔滤过的葡萄糖主要经表达于近端肾⼩管的SGLT2进⾏重吸收,卡格列净通过抑制SGLT2减少肾脏对滤过葡萄糖的重吸收,降低肾糖阈(RTG),增加尿糖排泄,从⽽降低⾎糖。
怡可安适应症:本品与⼆甲双胍联⽤:当单独使⽤⼆甲双胍⾎糖控制不佳时,可与⼆甲双胍联合使⽤,配合饮⾷和运动改善成⼈2型糖尿病患者的⾎糖控制。
治疗2型糖尿病的良药——卡格列净
治疗2型糖尿病的良药——卡格列净
邓迪大学的研究发现,一种新型已被批准用于治疗2型糖尿病的药物在没有二甲双胍合用的情况下也能取得很好疗效。
最近2年,美国和欧洲已经批准三种新型降糖药物——卡格列净、达格列净和依帕列净用于2型糖尿病的治疗。
这三种药物为钠-葡萄糖共同转运体2(SGLT2)抑制剂。
SGLT2是一种低亲和力、高载量的Na+葡萄糖转运体,主要位于近曲肾小管的S1和S2段,以1:1的比例偶联,主动转运肾小球过滤的钠和葡萄糖。
如果抑制这个过程,葡萄糖会在血液中减少,有利于糖尿病患者。
研究发现,卡格列净不仅能够抑制SGLT2,也可以激活腺苷酸活化蛋白激酶(AMPK),专家表示,达格列净和依帕列净没有做到这一点。
研究已经知道,二甲双胍可以通过激活AMPK发挥降糖作用,二甲双胍是治疗2型糖尿病的一线药物之一。
而卡格列净在激活AMPL的同时还以抑制SGLT2,这对于治疗2型糖尿病很好。
制药公司正在开展临床试验,以测试SGLT2抑制剂和二甲双胍合用的药效。
本次研究表明,卡格列净在单用时可能不需要再添加二甲双胍,因为卡格列净也可以激活AMPK。
整理卡格净列说明书_附件

附件192个药物临床试验数据自查核查注册申请清单附件1食品中二甲双胍等非食品用化学物质的测定BJS 201901•范围本标准规定了食品(含特殊食品)中二甲双胍、苯乙双胍、丁二胍、伏格列波糖、阿卡波糖、维达列汀、罗格列酮、西他列汀、吡格列酮、氯磺丙脲、达格列净、格列吡嗪、甲苯磺丁脲、醋磺己脲、妥拉磺脲、瑞格列奈、卡格列净、格列齐特、格列波脲、格列本脲、那格列奈、格列美脲、曲格列酮、格列喹酮、莫格他唑、GW501516、环格列酮等27种非食品用化学物质的高效液相色谱-串联质谱测定方法。
本标准适用于茶叶、奶粉、饼干、酒、饮料等食品(包括上述类似基质的片剂、胶囊剂等形式的特殊食品)中二甲双胍等27种非食品用化学物质的测定。
•原理试样粉碎后经甲醇超声提取,过滤后,上清液供高效液相色谱-串联质谱测定,外标法定量。
•试剂和材料除另有规定,本方法所用试剂均为分析纯或以上规格,水为GB/T 6682规定的一级水。
3.1 试剂3.1.1 乙腈(CH3CN):色谱纯。
3.1.2 甲酸(HCOOH):色谱纯。
3.1.3 甲酸铵(HCOONH4):色谱纯。
3.1.4 甲醇(CH3OH):分析纯。
3.2溶液配制3.2.1 0.1%甲酸水溶液:量取甲酸(3.1.2)1 mL,用水稀释至1000 mL,用滤膜(4.2)过滤后备用。
3.2.2 5 mmol/L甲酸铵水溶液:称取甲酸铵(3.1.3)0.315 g,用水稀释至1000 mL,用滤膜(4.2)过滤后备用。
3.2.3 5 mmol/L甲酸铵乙腈溶液:称取甲酸铵(3.1.3)0.315 g,加水50 mL溶解后,用乙腈稀释至1000 mL,用滤膜(4.2)过滤后备用。
3.3标准品苯乙双胍、丁二胍、二甲双胍、伏格列波糖、阿卡波糖、维达列汀、罗格列酮、西他列汀、吡格列酮、氯磺丙脲、达格列净、格列吡嗪、甲苯磺丁脲、醋磺己脲、妥拉磺脲、瑞格列奈、卡格列净、格列齐特、格列波脲、格列本脲、那格列奈、格列美脲、曲格列酮、格列喹酮、莫格他唑、GW501516、环格列酮标准品的中文名称、英文名称、CAS登录号、分子式、相对分子质量详见附录A中的表A.1,各标准品纯度均≥95%。
坎格列净片说明书简化版

Revised: XX/2013
8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy 8.3 Nursing Mothers 8.4 Pediatric Use 8.5 Geriatric Use 8.6 Renal Impairment 8.7 Hepatic Impairment
! Hypoglycemia: Consider a lower dose of insulin or the insulin secretagogue to reduce the risk of hypoglycemia when used in combination with INVOKANA (5.4)
10 OVERDOSAGE 11 DESCRIPTION 12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action 12.2 Pharmacodynamics 12.3 Pharmacokinetics 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of
------------------------------ADVERSE REACTIONS------------------------------! Most common adverse reactions associated with INVOKANA (5% or
greater incidence): female genital mycotic infections, urinary tract infection, and increased urination (6.1)
卡格列净片的功能主治
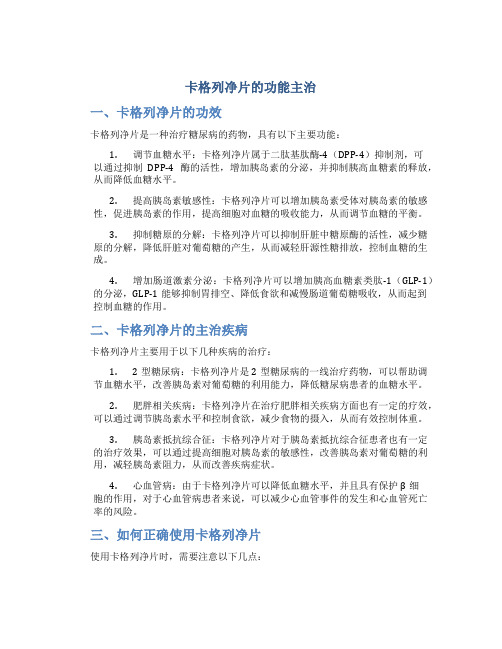
卡格列净片的功能主治一、卡格列净片的功效卡格列净片是一种治疗糖尿病的药物,具有以下主要功能:1.调节血糖水平:卡格列净片属于二肽基肽酶-4(DPP-4)抑制剂,可以通过抑制DPP-4酶的活性,增加胰岛素的分泌,并抑制胰高血糖素的释放,从而降低血糖水平。
2.提高胰岛素敏感性:卡格列净片可以增加胰岛素受体对胰岛素的敏感性,促进胰岛素的作用,提高细胞对血糖的吸收能力,从而调节血糖的平衡。
3.抑制糖原的分解:卡格列净片可以抑制肝脏中糖原酶的活性,减少糖原的分解,降低肝脏对葡萄糖的产生,从而减轻肝源性糖排放,控制血糖的生成。
4.增加肠道激素分泌:卡格列净片可以增加胰高血糖素类肽-1(GLP-1)的分泌,GLP-1能够抑制胃排空、降低食欲和减慢肠道葡萄糖吸收,从而起到控制血糖的作用。
二、卡格列净片的主治疾病卡格列净片主要用于以下几种疾病的治疗:1.2型糖尿病:卡格列净片是2型糖尿病的一线治疗药物,可以帮助调节血糖水平,改善胰岛素对葡萄糖的利用能力,降低糖尿病患者的血糖水平。
2.肥胖相关疾病:卡格列净片在治疗肥胖相关疾病方面也有一定的疗效,可以通过调节胰岛素水平和控制食欲,减少食物的摄入,从而有效控制体重。
3.胰岛素抵抗综合征:卡格列净片对于胰岛素抵抗综合征患者也有一定的治疗效果,可以通过提高细胞对胰岛素的敏感性,改善胰岛素对葡萄糖的利用,减轻胰岛素阻力,从而改善疾病症状。
4.心血管病:由于卡格列净片可以降低血糖水平,并且具有保护β细胞的作用,对于心血管病患者来说,可以减少心血管事件的发生和心血管死亡率的风险。
三、如何正确使用卡格列净片使用卡格列净片时,需要注意以下几点:1.按照医生的指导进行用药:在使用卡格列净片之前,一定要咨询医生并按照医生的指导进行用药,遵守用药的方法和剂量。
2.餐后服用:通常情况下,卡格列净片是餐后立即口服,建议在进餐后15分钟内服用。
3.副作用及注意事项:卡格列净片在使用过程中可能会引起一些副作用,如低血糖、胃肠道反应等,如果出现不适,应及时咨询医生处理。
格列净片的功能主治

格列净片的功能主治1. 什么是格列净片?格列净片是一种口服药片,主要成分是格列美脲(Gliclazide)。
它属于磺脲类口服降糖药物,用于治疗糖尿病。
2. 格列净片的功能主治格列净片主要用于控制和管理糖尿病,其功能主治包括以下几个方面:•控制血糖水平:格列净片通过促进胰岛素的分泌,降低胰岛素抵抗,从而帮助控制血糖水平。
它可以减少血糖在餐后的峰值,并降低空腹血糖水平。
•改善胰岛功能:格列净片能够增加胰岛素敏感性,提高胰岛细胞的功能,促进胰岛素的合成和释放,从而帮助控制血糖。
•减少胰岛素抵抗:糖尿病患者往往存在胰岛素抵抗现象,即细胞对胰岛素的敏感性降低。
格列净片可以增加细胞对胰岛素的敏感性,减少胰岛素的抵抗,提高胰岛素的利用率。
•保护胰岛细胞:格列净片还具有一定的保护胰岛细胞的作用,可以减少胰岛细胞的损伤和死亡,保护胰岛细胞的功能,延缓糖尿病的进展。
•降低心血管风险:糖尿病患者往往存在心血管疾病的风险。
格列净片可以通过控制血糖水平和改善胰岛功能,降低心血管疾病的发生风险。
3. 使用注意事项在使用格列净片的过程中,需要注意以下几个事项:•遵医嘱使用:格列净片属于处方药物,使用前需要遵循医生的建议和嘱托,按照医嘱剂量和频率进行使用。
•注意副作用:格列净片在使用过程中可能会出现一些副作用,如低血糖、胃肠道反应等。
如果出现副作用,应及时向医生咨询。
•避免过量使用:不要超过医生建议的剂量和频率,避免过量使用格列净片。
•与其他药物的相互作用:格列净片可能与其他药物发生相互作用,影响药效或出现不良反应。
在使用格列净片期间,应告知医生已经使用的其他药物。
•定期检查:在使用格列净片期间,应定期进行相关检查,包括血糖监测、肝功能检查等,以评估治疗效果和安全性。
4. 格列净片的禁忌症与注意事项在以下情况下,应当避免使用格列净片:•对格列美脲过敏:如果对格列美脲或者磺脲类药物过敏,应避免使用格列净片。
•糖尿病酮症酸中毒:格列净片不适合用于治疗糖尿病酮症酸中毒,需要在恢复后再考虑使用。
怡可安(Canagliflozin Tablets)说明书
核准日期:2017年09月29日修改日期:2019年06月27日2019年09月25日2020年03月16日2020年04月20日2020年06月24日2021年07月22日卡格列净片说明书请仔细阅读说明书并在医师指导下使用。
【药品名称】通用名称:卡格列净片商品名称:怡可安®英文名称:Canagliflozin Tablets汉语拼音:Kageliejing Pian【成份】主要成份:卡格列净化学名称:(1S)-1,5-脱水-1-C-(3-{[5-(4-氟苯基)噻吩-2-基]甲基}-4-甲基苯基)-D-葡萄糖醇化学结构式:分子式:C24H25FO5S 1/2 H2O分子量:453.53【性状】本品为黄色胶囊形薄膜衣片(100mg规格)或白色至类白色胶囊形薄膜衣片(300mg 规格),除去包衣后应显白色。
【适应症】本品与二甲双胍联用:当单独使用二甲双胍血糖控制不佳时,可与二甲双胍联合使用,配合饮食和运动改善成人2型糖尿病患者的血糖控制。
本品与二甲双胍和磺脲类药物联用:当联用二甲双胍和磺脲类药物血糖控制不佳时,可与二甲双胍和磺脲类药物联合使用,配合饮食和运动改善成人2型糖尿病患者的血糖控制。
本品不建议用于1型糖尿病患者或糖尿病酮症酸中毒(患者)的治疗。
【规格】(1)100mg;(2)300mg(以卡格列净无水物(C24H25FO5S)计)【用法用量】1. 开始本品治疗前在开始本品治疗前,应评估肾功能,并在治疗开始后定期进行评估。
(参见【注意事项】)对于既往未接受过本品治疗的血容量不足患者,开始本品治疗前建议纠正这种情况。
(参见【注意事项】、【老年用药】)2. 推荐剂量本品的推荐起始剂量为100mg每天一次,当天第一餐前服用。
对于耐受本品 100mg每天一次的剂量、肾小球滤过率估计值(eGFR)≥60mL/min/1.73m2且需要额外血糖控制的患者,剂量可增加至300mg每天一次(参见【注意事项】、【药理毒理】)。
药物卡格列净(Canagliflozin)合成检索总结报告
药物卡格列净(Canagliflozin)合成检索总结报告
一、卡格列净(Canagliflozin)简介
卡格列净(Canagliflozin)于2013年3月29日在美国上市。
卡格列净(Canagliflozin)是FDA批准上市的第一个钠-葡萄糖共转运蛋白2抑制剂。
卡格列净(Canagliflozin)适用于2型糖尿病的成人患者。
卡格列净(Canagliflozin)不良反应:女性生殖器霉菌感染、尿道感染、多尿。
卡格列净(Canagliflozin)分子结构式如下:
英文名称:Canagliflozin
中文名称:卡格列净
本文主要对卡格列净(Canagliflozin)的合成路线、关键中间体的合成方法及实验操作方法进行了文献检索并作出了总结。
二、卡格列净(Canagliflozin)合成路线一
三、卡格列净(Canagliflozin)合成路线二
四、卡格列净(Canagliflozin)合成路线三
五、卡格列净(Canagliflozin)合成路线四
六、卡格列净(Canagliflozin)合成路线一检索总结报告(一) 卡格列净(Canagliflozin)中间体2的合成(路线一)
(二) 卡格列净(Canagliflozin)中间体4的合成(路线一)。
卡格净列说明书
【药品名称】通用名称:卡格列净片商品名称:卡格列净片(怡可安)英文名称:Canagliflozin Tablets拼音全码:KaGeLieJingPian(YiKeAn)【主要成份】主要成份:卡格列净。
【性状】本品为黄色胶囊形薄膜衣片(100mg规格)或白色至类白色胶囊形薄膜衣片(300mg规格)。
除去包衣后应显白色。
【适应症/功能主治】本品与二甲双胍联用:当单独使用二甲双胍血糖控制不佳时,可与二甲双胍联合使用,配合饮食和运动改善成人2型糖尿病患者的血糖控制。
本品与二甲双胍和磺脲类药物联用:当联用二甲双胍和磺脲类药物血糖控制不佳时,可与二甲双胍和磺脲类药物联合使用,配合饮食和运动改善成人2型糖尿病患者的血糖控制。
本品不建议用于1型糖尿病患者或糖尿病酮症胺中毒(患者)的治疗。
【规格型号】 100mg*10s*1板【用法用量】本品的推荐起始剂量为100mg每天一次,当天第一餐前服用。
对于耐受本品100mg每天一次的剂量、肾小球滤过率估计值(eGFR) ≥60 mL/min/1.73 m2且需要额外血糖控制的患者,剂量可增加至300mg每天一次(参见注意事项、药理毒理)。
对于血容量不足的患者,开始本品治疗前建议纠正这种情况(参见注意事项、老年用药)。
肾损害患者在开始本品治疗前,建议评估肾功能,并在治疗开始后定期进行评估。
轻度肾损害(eGFR≥60 mL/min/1.73 m2)的患者无需调整剂量。
对于中度肾损害(eGFR≥45至<60 mL/min/1.73 m2)的患者,本品的剂量限制为100mg每天一次。
对于eGFR<45mL/min/1.73 m2的患者,不建议使用本品。
当eGFR持续低于45 mL/min/1.73 m2时,不建议使用本品(参见注意事项)。
eGFR低于30 mL/min/1.73 m2的患者禁止使用本品(参见注意事项)。
肝损害患者轻度至中度肝损害患者无需调整剂量。
目前没有在重度肝损害患者中开展I临床研究,故不推荐重度肝损害的患者使用本品。
卡格列净的功能主治
卡格列净的功能主治什么是卡格列净?卡格列净(Kagglegin),是一种常用的中成药,具有很多的功效和主治作用。
它由多种中药组合而成,经过科学配方和严格制作工艺而成。
下面将介绍卡格列净的功能主治。
卡格列净的功能卡格列净具有以下功能:1.清热解毒:卡格列净具有清热解毒的作用,可以清除体内的热毒素,提高身体的抵抗力,减少疾病的发生。
2.消肿止痛:卡格列净能够起到消肿止痛的作用,可以缓解疼痛和不适感,减轻肿胀和红肿症状。
3.灭菌消炎:卡格列净具有良好的灭菌消炎作用,可以抑制细菌的生长和繁殖,减少炎症反应,促进伤口的愈合。
4.利尿通淋:卡格列净能够促进尿液的排出,增加尿量,有利于清除体内的废物和毒素,预防尿路感染的发生。
5.调节免疫:卡格列净可以调节免疫系统的功能,提高机体的抵抗力,增强免疫力,预防疾病的发生。
6.缓解痛经:卡格列净对于一些痛经症状也有一定的缓解作用,可以减轻腹痛和腰痛的程度,改善女性的经期不适感。
主治作用根据卡格列净的功能,它的主治作用包括但不限于以下几种:1.感冒发热:卡格列净可以用于治疗感冒引起的发热、咳嗽、喉咙痛等症状。
它可以清除体内的病毒和热毒素,减轻症状,促进康复。
2.口腔溃疡:卡格列净可以用于治疗口腔溃疡引起的疼痛和不适感。
它具有消炎杀菌的作用,可以减轻口腔溃疡的炎症,促进愈合。
3.尿路感染:卡格列净可以用于治疗尿路感染引起的尿频、尿急、尿痛等症状。
它具有利尿通淋的作用,可以清除尿路的细菌和废物,缓解症状。
4.痛经症状:卡格列净可以用于缓解痛经引起的腹痛、腰痛等不适感。
它可以调节免疫系统的功能,减少子宫收缩引起的疼痛。
5.皮肤病:卡格列净可以用于治疗一些皮肤病引起的瘙痒、红斑、水疱等症状。
它具有清热解毒的作用,可以改善皮肤炎症,减轻症状。
使用注意事项使用卡格列净时,需要注意以下事项:1.请遵医嘱使用:使用卡格列净前,请咨询医生或药师的意见,并按照医嘱使用,不要超过推荐剂量。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
CENTER FOR DRUG EVALUATION ANDRESEARCHAPPLICATION NUMBER:204042Orig1s000OFFICE DIRECTOR MEMORegarding safety, a cardiovascular (CV) meta-analysis safety review determined a potential risk signal of harm for those receiving therapy within the first 30 days with a neutral effect after 30 days. Also noted were potential decreases in GFR in those with compromised renal function, and effects on bone remodeling. These issues will be discussed further later in this review.DMEP is recommending that this application receive an Approval action. I agree with this recommendation and will discuss reasoning and conclusions below.EfficacyCanagliflozin 300 mg and 100 mg was compared to placebo in HbA1c change from baseline for superiority in monotherapy and as add-on therapy to other anti-hyperglycemic agents (AHA) in a variety of patient populations. There also were non-inferiority comparisons with marketed anti-diabetic drugs. Below is a table from Dr. Liu’s review summarizing the efficacy results (Page 6-7).Table 1. Primary Efficacy Results (HbA1c) for Canagliflozin (300 mg and 100 mg) in Patients with Type 2 Diabetes (Phase 3 Studies) (mITT/LOCF)Study (Weeks) Treatment arm n BaselineMean ± SE LSMeanchange ± SECanaglifozin minuscontrol (95% CI)p-valueMonotherapyDIA3005 (26) Main study Cana 300 mgCana 100 mgPlacebo1931911898.01 ± 0.078.06 ± 0.077.97 ± 0.07-1.03 ± 0.06-0.77 ± 0.060.14 ± 0.06-1.16 (-1.34, -0.99)-0.91 (-1.09, -0.73)<.0001<.0001DIA3005 (26) High Glycemic Cana 300 mgCana 100 mg434610.62 ± 0.1510.59 ± 0.13-2.56±0.22-2.13±0.22Add-on to AHA MonotherapyDIA3006 (26) Add-on to metformin Cana 300 mgCana 100 mgPlacebo3603651817.95 ± 0.057.94 ± 0.057.96 ± 0.07-0.94 ± 0.04-0.79 ± 0.04-0.17 ± 0.06-0.77(-0.91,-0.64)-0.62 (-0.76,-0.48)<.0001<.0001DIA3009 (52) Add-on to metform Cana 300 mgCana 100 mgGlimepiride↑6/8 mg4744784737.79 ± 0.047.78 ± 0.047.83 ± 0.04-0.93 ± 0.04-0.82 ± 0.04-0.82 ± 0.04-0.12 (-0.22, -0.02)-0.01 (-0.11, 0.09)0.01580.8074Add-on to Dual Combination AHA TherapyDIA3002 (26)+ metformin + sulfonylurea Cana 300 mgCana 100 mgPlacebo1521551508.13 ± 0.088.13 ± 0.078.12 ± 0.07-1.06 ± 0.08-0.85 ± 0.08-0.13 ± 0.08-0.92 (-1.11, -0.73)-0.71 (-0.90, -0.52)<.0001<.0001DIA3012 (26) +metformin Cana 300 mgCana 100 mg1121137.84 ± 0.097.99 ± 0.09-1.03 ± 0.07-0.89 ± 0.07-0.76 (-0.95, -0.57)-0.62 (-0.81, -0.44)<.0001<.0001+ pioglitazone Placebo 114 8.00 ± 0.09 -0.26 ± 0.07DIA3015 (52) +metformin + sulfonylurea Cana 300 mgSitagliptin100mg3653748.13 ± 0.058.12 ± 0.05-0.66 ± 0.05-1.03 ± 0.05-0.37 (-0.50, -0.25) <.0001Special PopulationDIA3010(26)1 older adults Cana 300 mgCana 100 mgPlacebo2292392327.69 ± 0.057.77 ± 0.057.76 ± 0.05-0.73 ± 0.06-0.60 ± 0.06-0.03 ± 0.06-0.70 (-0.84, -0.57)-0.57 (-0.71, -0.44)<.0001<.0001DIA3004 (26)2 Moderate renal impairment Cana 300 mgCana 100 mgPlacebo8988877.97 ± 0.097.89 ± 0.108.02 ± 0.10-0.44 ± 0.09-0.32 ± 0.09-0.03 ± 0.09-0.42 (-0.65, -0.19)-0.29 (-0.53, -0.06)0.00040.0131DIA3008 (18) Sulphonylurea substudy3Cana 300 mgCana 100 mgPlacebo3940408.28 ± 0.168.29 ± 0.138.49 ± 0.18-0.79 ± 0.15-0.70 ± 0.150.04 ± 0.15-0.83 (-1.24, -0.42)-0.74 (-1.14, -0.33)0.00010.0005DIA3008 (18) Insulin substudy2Cana 300 mgCana 100 mgPlacebo5725515458.27 ± 0.048.34 ± 0.048.24 ± 0.04-0.72 ± 0.03-0.63 ± 0.030.02 ± 0.03-0.74 (-0.82, -0.65)-0.65 (-0.74, -0.56)<.0001<.00011≥55 to ≤80 years of age 2 eGFR ≥ 30 to <50 mL/min/1.73 m23 population 14 population 2Canagliflozin 300 mg and 100 mg demonstrated significant efficacy in all placebo comparisons. Both doses of canagliflozin were non-inferior to glimepiride and sitagliptin when using a non-inferiority margin of 0.3%. Placebo-subtracted change from baseline in HbA1c was -0.91 and -1.16 for the 100 and 300 mg doses, respectively, when used as monotherapy. When added to other anti-diabetic medications the treatment difference ranged from -0.62 to -0.92. Canagliflozin 300 mg demonstrated superiority to glimepiride (Study 3009) and to sitagliptin 100 mg (Study 3015) at 52 weeks.Canagliflozin 300 mg demonstrated numerically greater point estimate changes than canagliflozin 100 mg on HbA1c (0.1% to 0.25% depending on population studied) in all studies.Canagliflozin demonstrated modest efficacy in subjects with moderate renal impairment (Study 30042-Dr. Liu’s review, page 34-35).Table 7.2 Primary Efficacy Results in DIA3004Endpoint Placebo Canagliflozin 100mg Canagliflozin 300mgHbA1c (%) n n nBaseline mean ± SEAdj. Mean Change from baseline±SE LOCF* (by sponsor)MMRM 8787858.02 ± 0.10-0.03 ± 0.09-0.10 ± 0.088888847.89 ± 0.10-0.33 ± 0.09-0.33 ± 0.088989857.97 ± 0.09-0.44 ± 0.09-0.48 ± 0.082 GFR ≥30 and <50 mL/min/1.73m2PP* (by sponsor)Cana−P, adjusted LS Mean (95% CI) LOCF* (by sponsor)MMRMPP* (by sponsor) 63 -0.16 ± 0.10 67 -0.32 ± 0.10-0.30 (-0.53, -0.07)-0.23 (-0.44, -0.02)-0.17 (-0.42, 0.09)77 -0.48 ± 0.09-0.40 (-0.63, -0.17)-0.38 0.58, -0.17)-0.33 (-0.57, -0.08)Patients (%) achieving HbA1c <71,2 LOCF1sponsor’s results (LOCF) 3 8(11%)10 (13%)15 (17%)15(20%)18 (24%)24 (27%)21(25%)23 (28%)29 (33%)Integrated analysis of efficacy results from subjects with moderate renal impairment was performed across several trials to allow for a larger database and further stratification of efficacy based on GFR (Dr. Parks’ review, page 9).Table 7.3. Integrated Analysis of HbA1c Reduction in Patients with Moderated Renal ImpairmentHbA1c (%) Placebo Canagliflozin 100mg Canagliflozin 300mgeGFR ≥30 to 60 mL/min/1.73 m2n n nBaseline mean ± SEAdj. Mean Change from baseline±SE LOCF *(by sponsor)PPCana−P, adjusted LS Mean (95% CI) LOCF* (by sponsor)PP 3563562897.98 ± 0.05-0.14 ± 0.06-0.32 ± 0.063263262858.09 ± 0.05-0.52 ± 0.06-0.63 ± 0.06-0.38 (-0.50, -0.26)-0.31 (-0.44, -0.18)3543543098.07 ± 0.05-0.62 ± 0.06-0.72 ± 0.06-0.47 (-0.60, -0.35)-0.40 (-0.53, -0.28)eGFR < 45 mL/min/1.73 m2n n nBaseline mean ± SEAdj. Mean Change from baseline±SE LOCF* (by sponsor)PPCana−P, adjusted LS Mean (95% CI) LOCF* (by sponsor)PP 108108858.10 ± 0.090.05 ± 0.19-0.48 ± 0.25118118928.08 ± 0.09-0.18 ± 0.19-0.76 ± 0.26-0.23 (-0.45, -0.01)-0.28 (-0.53, -0.03)1221221068.10 ± 0.08-0.34 ± 0.19-0.84 ± 0.26-0.39 (-0.61, -0.17)-0.36 (-0.61, -0.12)eGFR ≥ 45 mL/min/1.73 m2n n nBaseline mean ± SEAdj. Mean Change from baseline±SE LOCF* (by sponsor)PP okCana−P, adjusted LS Mean (95% CI) LOCF* (by sponsor)PP 2482482047.98 ± 0.06-0.10 ± 0.07-0.28 ± 0.072082081938.11 ± 0.06-0.57 ± 0.07-0.61 ± 0.07-0.47 (-0.61, -0.32)-0.34 (-0.49, -0.18)2322322038.10 ± 0.06-0.62 ± 0.07-0.72 ± 0.07-0.52 (-0.66, -0.38)-0.44 (-0.59, -0.29)This analysis demonstrates that as GFR decreases, so to do reductions in HbA1c with placebo-subtracted reductions in HbA1c of approximately 0.5% for subjects with GFR ≥ 45 to < 60mL/min/1.73m2 and placebo-subtracted mean reduction of 0.2 to 0.4% for subjects with eGFR ≥30 to < 45 mL/min/1.73m2. These results will need to be viewed in the context of any potential safety issues in these populations.To provide information on the efficacy of canagliflozin in a larger group of T2DM subjects with moderate renal impairment, a population of subjects with a baseline eGFR of ≥30 to <60 mL/min/1.73m2 were examined (Dr. Liu’s review, page 41-42).Table 3.2.5.1. Results for Canagliflozin (300 mg and 100 mg) in Patients with Type 2 Diabetes with Moderate Renal Impairment (eGFR ≥30 to <60 mL/min) (mITT/LOCF)HbA1c (%) Placebo Canagliflozin 100mg Canagliflozin 300mgeGFR ≥30 to 60 mL/min/1.73 m2n n nBaseline mean ± SEAdj. Mean Change from baseline±SE LOCF *(by sponsor)PPCana−P, adjusted LS Mean (95% CI) LOCF* (by sponsor)PP 3563562897.98 ± 0.05-0.14 ± 0.06-0.32 ± 0.063263262858.09 ± 0.05-0.52 ± 0.06-0.63 ± 0.06-0.38 (-0.50, -0.26)-0.31 (-0.44, -0.18)3543543098.07 ± 0.05-0.62 ± 0.06-0.72 ± 0.06-0.47 (-0.60, -0.35)-0.40 (-0.53, -0.28)eGFR < 45 mL/min/1.73 m2n n nBaseline mean ± SEAdj. Mean Change from baseline±SE LOCF* (by sponsor)PPCana−P, adjusted LS Mean (95% CI) LOCF* (by sponsor)PP 108108858.10 ± 0.090.05 ± 0.19-0.48 ± 0.25118118928.08 ± 0.09-0.18 ± 0.19-0.76 ± 0.26-0.23 (-0.45, -0.01)-0.28 (-0.53, -0.03)1221221068.10 ± 0.08-0.34 ± 0.19-0.84 ± 0.26-0.39 (-0.61, -0.17)-0.36 (-0.61, -0.12)eGFR ≥ 45 mL/min/1.73 m2n n nBaseline mean ± SEAdj. Mean Change from baseline±SE LOCF* (by sponsor)PP okCana−P, adjusted LS Mean (95% CI) LOCF* (by sponsor)PP 2482482047.98 ± 0.06-0.10 ± 0.07-0.28 ± 0.072082081938.11 ± 0.06-0.57 ± 0.07-0.61 ± 0.07-0.47 (-0.61, -0.32)-0.34 (-0.49, -0.18)2322322038.10 ± 0.06-0.62 ± 0.07-0.72 ± 0.07-0.52 (-0.66, -0.38)-0.44 (-0.59, -0.29)* This reviewer obtained the same results as the sponsorThese findings, which include data from Studies DIA3004, DIA3005, DIA3008 and DIA3010, were similar to the findings of DIA3004 alone.A variety of secondary endpoints were also evaluated as documented in other reviews. Some of interest includes end of study body weight, systolic blood pressure (SBP) and change in fasting serum lipid parameters. There are numerical changes in body weight and SBP favoring canagliflozin, usually dose related, in the studies.Dr. Kwon has a nice summary of the efficacy results (Page 62-63):The largest HbA1c reduction associated with canagliflozin was seen in monotherapy trial (DIA3005), where canagliflozin 100 mg and 300 mg achieved -0.91% and -1.16% difference from placebo. The following points summarize the range of glycemic efficacy across other Phase 3 trials:•Canagliflozin 100 mg and 300 mg, when added to metformin background therapy, achieved a range of -0.62 to -0.77% difference from placebo in HbA1c reduction(DIA3006)•Canagliflozin 100 mg and 300 mg, when added to sulfonylurea background therapy, achieved a range of -0.74 to -0.83% difference from placebo in HbA1c reduction(DIA3008 SU substudy)•Canagliflozin 100 mg and 300 mg, when added to metformin and SU background therapy, achieved a range of -0.71 to -0.92% difference from placebo in HbA1creduction (DIA3002)•Canagliflozin 100 mg and 300 mg, when added to metformin and pioglitazone background therapy, achieved a range of -0.62 to -0.76% difference from placebo inHbA1c reduction (DIA3012)•Canagliflozin 100 mg and 300 mg, when added to background insulin therapy, achieved a range of -0.65 to -0.74% difference from placebo in HbA1c reduction(DIA3008 Insulin substudy)As discussed above, canagliflozin 300 mg and 100 mg demonstrated statistically significant changes in HbA1c from placebo in a variety of different patient populations. There was a dose-response mean reduction in HbA1c of 0.1% to 0.25% depending upon the population studied. Canagliflozin 300 mg demonstrated non-inferiority and statistical superiority to sitagliptin and glimepiride in the populations studied. Efficacy decreased with decreasing renal function. Important secondary endpoints supported the findings in the primary endpoint. There were dose-related numerical decreases in weight3 and blood pressure4 in all studies favoring canagliflozin therapy.SafetyThe main safety issues to consider are CV safety5, renal safety, bone effects, osmotic diuresis and potential for resultant dehydration. Canagliflozin also increases urinary glucose excretion3 0.4-3.3% placebo adjusted percent reduction depending upon the trial with some dose response. Dual X-ray absortiometry and computed tomography suggest weight loss was predominantly due to fat mass loss both from visceral and subcutaneous compartments.4 0.1-8 mm Hg depending on trial and dose. There was some dose response.5 While Canagloflozin use is associated with decreased weight and BP, it is also associated with increase in LDL of -2 to +8.5% for the 100 mg dose and +2.8 to +12% for the 300 mg dose.with resultant increases in urinary tract infections, a known effect that I will not discuss further.Cardiovascular SafetyAll non-insulin diabetic drugs seeking approval for use in T2DM are required to undergo evaluation to demonstrate that they do not increase CV risks. Canagliflozin use is associated with decreases in weight and blood pressure which if there are not other off-target effects could be viewed, at the very least, as effects that would not increase the risk for cardiovascular events. However, canagliflozin use is associated with increases in pooled placebo-adjusted LS mean LDL of 5.7% and 9.3% with the 100 mg and 300 mg doses, respectively.The sponsor evaluated CV safety through a meta-analysis of 9 randomized, controlled trials. These trials included an interim analysis from a dedicated cardiovascular outcomes trial (CVOT) known as CANVAS. The data from CANVAS was unblinded by the sponsor and presented at the Advisory Committee Meeting and as I will discuss below brings up issues of whether CANVAS can continue and be relied upon for further evaluation of CV risk. Canvas had a total sample size of 4330 subjects, with 1442, 1445 and 1443 subjects assigned to placebo, canagliflozin 100 mg and canagliflozin 300 mg, respectively.6 The primary safety endpoint was major adverse cardiovascular events plus (MACE plus; CV death, non-fatal MI, non-fatal stroke and hospitalizations due to unstable angina =201 events). There were 130 MACE-plus events in the canagliflozin treatment group and 71 MACE-plus events in the comparator group. CANVAS contributed 108 and 53 (≈80%) of these events in the canagliflozin and comparator groups, respectively. Below are the results in tables taken from Dr. Andraca-Carrera’s review (Page 3, 4-5).Table 1. Primary and Secondary Analyses of MACE-plusCanagliflozin (events / N) Comparators(events / N)Hazard Ratio(95% CI)Primary Analysis (including all 9 trials)130 / 6396 71 / 3327 0.91 (0.68, 1.21)7 Secondary AnalysesFirst 30 Days in CANVAS 13 / 2886 1 / 1441 6.49 (0.85, 49.64) After first 30 Days in CANVAS 95 / 2867 52 / 1435 0.89 (0.64, 1.25) Non-CANVAS trials 22 / 3510 18 / 1886 0.64 (0.34, 1.19) Source: Created by reviewer. Dataset: adttecv.xpt6 Inclusion criteria: men or women with a diagnosis of T2DM, HbA1c levels ≥7% and ≤10.5% at screening, either (1) not on antihyperglycemic agent (AHA) therapy or (2) on AHA monotherapy or combination therapy with any approved agent, history or high risk of CV disease defined as either (1) age ≥ 30 with documented symptomatic atherosclerotic CV disease or (2) age ≥ 50 with 2 or more risk factors for CV disease7 The 99.9% confidence interval to rule out 1.3 for the interim analysis is 0.56, 1.48).Table 2. Components of MACE-plus in All Trials in the Meta-analysisCanagliflozin N= 6396ComparatorsN = 3327Hazard Ratio(95% CI)MACE 104 53 0.98 (0.70, 1.36)CV Death 21 16 0.65 (0.34, 1.24)MI 45 27 0.83 (0.51, 1.34)Stroke 47 16 1.46 (0.83, 2.58) Hospitalized unstable angina 26 18 0.71 (0.39, 1.30)Source: Created by reviewer. Dataset: adttecv.xptAs the first table above demonstrates, the upper bound of the 95% confidence interval is below the risk margin of 1.8 necessary for adequate CV safety to allow marketing (for this specific issue). As noted above, there was an imbalance of MACE-plus events in the first 30 days not favoring canagliflozin in the total database and in CANVAS itself, but not in the meta-analysis when excluding CANVAS. Although at the Advisory Committee (AC) meeting, some panel members proposed possible biologically explanations as to why this may be a real finding, others felt this likely due to chance. The 30 day results are based on 14 events (canagliflozin 100 mg-7 events, canagliflozin 300 mg-6 events), recognizing the approximate 2:1 randomization8 so there are essentially 7 events to 1. The small number of events, lack of dose-response, sensitivity of hazard ratio to small changes in the number of events in the comparator arm9, and fewer events in the comparator arm than would be anticipated based on the overall rate make interpretation of the validity of this result (real vs. chance) difficult if not impossible. This certainly was not a sustained finding as results from further exposure did not demonstrate CV harm, and we have not found a specific population based on the 14 events that seems at greater risk of harm.10The estimated hazard ratio and 95% confidence interval for MACE is 0.98 (0.70, 1.36) also demonstrating no evidence of increased risk associated with canagliflozin. Noted above is that stroke has a point estimate of 1.46 and is the only component of MACE with a point estimate that is not less than one. The estimated hazard ratio and 95% confidence interval for the primary endpoint MACE-plus and MACE associated with canagliflozin in the 8 trials excluding CANVAS was 0.64 (0.34, 1.19) and 0.63 (0.32, 1.25), respectively.However, CANVAS was a dedicated study which may give more validity to the cardiovascular findings if they are in conflict with the meta-analysis. It is interesting to note that the imbalance for stroke noted above in the overall meta-analysis is not present in the analysis of CANVAS by itself as noted in the table below from Dr. Parks’ review (Page 17).8 Canaglizozin N=6396 (6876 pt-yrs), comparator N=3327 (3470 pt-yrs).9 Expected number of comparator events was 3.76 during first 30 days. 1and 3 additional events in thecomparator arm would result in hazard ratio and 95% CI of 3.25 (0.73, 14.38) and 1.62 (0.53, 4.97) respectively 10 The first post-randomization visit was scheduled for 12-weeks and there was no systematic planned within trialassessment at one month . Those with the early events did not have distinguishing features to identify a subpopulation, or particular reaction to the medication (dehydration, hypoglycemia) that may lend credibility to this being a real finding. Mean age, sex HbA1c levels, baseline eGFR, LDL-C, BMI, previous history of CV disease, CV risk factors, Diabetes >/=10 years, SBP >140 mmHg and micro-albuminuria were all similar in those with events within and after 30 days.It is also interesting to note the contradiction between CV death and MI and MI between the meta-analysis and CANVAS. All of the various disparate results noted between meta-analysis and comparison to CANVAS illustrate the need for complete data from a dedicated trial.The sponsor plans to exclude a risk margin of 1.3 after 500 and 700 MACE-plus events in the canagliflozin development program through a meta-analysis of several disparate trials. This will not be acceptable from the standpoint that the 1.3 risk margin should be evaluated from what would essentially be considered a stand-alone trial. Therefore, the events used in the final evaluation should come solely from CANVAS or something similar. Additionally, MACE-plus will not be an acceptable primary endpoint. While we have been willing to accept some discretion in the choice of endpoint for 1.8 in the interest of not unduly delaying access to effective drugs, for the 1.3 goalpost we want more certainty that ‘truth’ is being represented. We are concerned that the further evaluations stray from more objective criteria of strict MACE (CV death, non-fatal MI, non-fatal stroke), the more ‘noise’ is introduced into the evaluation which may bias results toward non-inferiority. Therefore, we have been requiring strict MACE as the endpoint in CVOT trials to demonstrate a risk margin less than 1.3 which would allow continued marketing.The CV information above is adequate to demonstrate safety that would allow marketing for this specific issue. However, unblinding of the CVOT and public disclosure of interim results brings up a number of issues that must be grappled with regarding whether the unblinding could affect the conduct of the trial so as to invalidate final results. While there is much concern that investigator or participant behaviors could be affected such that bias may be introduced (initial favorable results may drive those on study to seek off-study drug, unfavorable results may cause unbalanced withdrawal from study corrupting evaluation arms), there also are not many (or perhaps any) examples to validate these concerns. Things that may make unblinding less concerning are that the CVOT was fully enrolled at the time of public disclosure and the point estimate for MACE was essentially unity. In reality, it will not truly be known what, if any, impact the public disclosure had unless the trial is finalized and the database fully reviewed.In order for the sponsor to fully comply with a completed CVOT analysis fulfilling the 1.3 upper bound margin that will allow continued marketing, they will need to have a stand-alone trial, not a meta-analysis of many disparate trials. The analysis showing an upper bound of 1.3 will also need to be based on strict MACE, and not MACE+. This may be accomplished byas volume status stabilizes. These results have to be viewed under the context that as renal function declines, so does efficacy of canagliflozin.Because of canagliflozin action as an osmotic diuretic, increases in urinary output may lead to volume contraction and volume-related events. The incidence of osmotic diuresis did not appear to be dose-dependent whereas the incidence of volume depletion appeared to be dose-dependent with elderly (≥75 years) subjects with low baseline renal function (<60mL/min/1.73m2) using loop diuretics at greatest risk.To evaluate the effect of canagliflozin on GFR, baseline renal function in the impaired range was stratified according to two categories: GFR ≥45 to 60 mL/min/1.73m2 and GFR ≥30 to 45 mL/min/1.73m2. The mean reduction in GFR from baseline was between 1 and 5 ml/min/1.73 m2 depending upon dose for the group whose GFR at baseline was 45-60 mL/min/1.73m2.14 An inconsistent pattern is demonstrated for the group whose baseline GFR was ≥30 to 45mL/min/1.73m2, likely due to a smaller sample size, but the absolute decrease appears to be approximately the same as that of the GFR > 45 to 60 mL/min/1.73m2 group , which based on a lower initial GFR represents a greater percentage of functional decrease.Categorical changes based on GFR are presented in the table below from Dr. Parks’ review (Page 24).Table 8.2 Change in eGFR by Baseline Renal Status; n (%) from DS3Control Cana 100 Cana 300> 60 ml/kg/1.73 m2>30% decrease (anyvalue)162/2739 (5.9%) 146/2643 (5.5%) 225/2583 (8.7%)>30% decrease (lastvalue)67 (2739 (2.4%) 57/2643 (2.2%) 84/2583 (3.3%)>50% decrease (anyvalue)16/2739 (0.6%) 14/2643 (0.5%) 23/2583 (0.9%)>50% decrease (lastvalue)6/2739 (0.2%) 1/2643 (<0.1%) 9/2583 (0.3%)45-60 ml/kg/1.73 m2>30% decrease (anyvalue)21/300 (7%) 23/252 (9.1%) 34/255 (13.3%)>30% decrease (lastvalue)6/300 (2.0%) 9/252 (3.6%) 13/255 (5.1%)>50% decrease (any value) 0 4/252(1.6%) 0>50% decrease (last value) 0 1/252(0.4%) 030-45 ml/kg/1.73 m2>30% decrease (anyvalue)12/114 (10.5%) 24/121 (19.8%) 27/123 (22%) 14 Based on data from DIA3008.>30% decrease (lastvalue)6/114 (5.3%) 9/121 (7.4%) 9/123 (7.3%)>50% decrease (anyvalue)0 2/121 (1.7%) 4/123 (3.3%)>50% decrease (last value) 0 1/121(0.8%) 0Source: Applicant’s 3/15/13 response to FDA information requestThe results above demonstrate again that as GFR decrease, categorical increases in >30% decreases occur.As there is a lingering question regarding the effect of canagliflozin on renal function, and given the marginal meaningful benefit in those with renal function <45 ml/kg/1.73 m2, it seems reasonable to exclude this group from therapy. In those with GFR ≥45 to 60mL/min/1.73m2 canagliflozin does have efficacy, but also seems to have dose related decreases in GFR. Therefore, given the small amount of efficacy between doses, it would be reasonable to limit the dose in this group to 100 mg a day.Advisory Committee MeetingAn advisory committee meeting was held on January 10, 2013. Most of the discussion pertained to the assessment of CV safety, renal safety. As noted before, panel members discussed the potential for CV disadvantage for the first 30 days of use but there wasn’t consensus with views ranging from chance finding to potential biologic plausibility. Concern was voiced whether the disclosure of the interim results of CANVAS would invalidate the final results.Discussions regarding renal safety were focused on whether there should be limitations placed on use in those with moderate to severe renal function due to the safety findings and waning efficacy.The panel members voted 10 to 5 on the question, “Based on the information included in the briefing materials and presentations today, has the applicant provided sufficient efficacy and safety data to support marketing of canagliflozin for the treatment of Type 2 diabetes mellitus?”Conclusions and RecommendationsCanagliflozin has demonstrated efficacy for the 300 and 100 mg per day dose in the overall population with an indication of a small increase of mean effect with increased dose. As renal function decreases, so too does the efficacy such that the effect for those with GFR <45mL/min/1.73m2 is marginal. There also seems to be increasing adverse effect with increasing dose.There are lingering questions regarding canagliflozin’s effect on renal function, which seems the most pronounced in those with GFR <45 mL/min/1.73m2 such that these patients shouldnot receive therapy until more is known. Because of the possible dose-effect on GFR, those patients with GFR 45-60 mL/min/1.73m2 should not exceed 100 mg per day. Also, since there seems to be dose-related adverse events and a marginal increased in mean efficacy with higher doses, the starting dose should be 100 mg per day in all subjects with dose escalation for those that require more intensive therapy (with the exceptions for those with renal compromise as discussed above).The sponsor will have to complete the PMRs as noted in other reviews and with agreed upon labeling I recommend an approval action.。