前臂双骨折的手术入路
前臂骨折的固定方式与手术入路骨科基础
前臂骨折的固定方式与手术入路骨科基础进行夹板和臂夹板等外固定可以保护患肢,避免进一步的软组织损伤。
存在开放骨折时,清洗伤口,进行X线检查,无菌敷料包扎直至患者手术。
多种损伤机制都可以造成前臂骨折。
对于不同人群和损伤类型,治疗方式各不相同。
成人骨骼无重塑能力,且其前臂功能上更像是一个关节,所以治疗的目的是达到解剖复位和固定,使残留畸形和功能受损最小化。
切开复位内固定术适用于除前臂单骨完全无移位骨折以外的所有骨折。
应用拉力螺钉和中和钢板或加压钢板获得绝对稳定可以实现直接骨愈合。
软组织情况和骨折类型无法实现绝对稳定时,可以考虑应用桥接钢板。
临时外架固定常会导致功能不良,可以作为二线治疗方式。
手法复位和石膏制动手法复位和石膏制动不能用于治疗承认前臂损伤。
成年人骨膜较薄,骨折手法复位后难以保持前臂双骨折的位置。
石膏制动只能用于无位移和轻微肿胀的患者。
对这类患者需要经常随访,他们可能会有轻度功能不良,有位置丢失或不愈合手术干预的风险。
1钢板钢板是固定的一种类型,而不是固定的模式或愈合的类型。
在前臂骨折中,钢板有很多种使用方式,在治疗前明确钢板使用的目的非常重要。
对成人移位骨折的常规处理是进行绝对稳定固定。
对斜形骨折可以使用拉力螺钉和钢板获得绝对稳定固定。
横向骨折时需要使用加压钢板。
术前计划很重要,外科医师在手术前应决定钢板的类型和使用方法。
在正常前臂骨折中,传统螺钉足以胜任。
应该使用标准的加压钢板。
比之轻1/3的管型钢板不能应用于成人前臂骨干骨折,可以应用于小儿骨折。
以上述方式使用加压钢板可以取得良好的骨折愈合率,在成人和儿童中并发症的风险很低。
对前臂广泛粉碎性骨折和(或)软组织损伤可以应用桥接钢板。
这种情况下试图取得绝对稳定会破坏骨块血运,引起骨折不愈合。
虽然无法实行解剖复位,但对桡骨和尺骨整体的解剖排列很有必要,可以避免旋前旋后功能不良。
应用桥接钢板时,手术医师在试图维持骨块血运、促进骨折愈合时要接受一定程度上的功能不良。
骨科基础图文详解:桡骨前侧入路
骨科基础图文详解:桡骨前侧入路桡骨前侧入路可以良好而安全地显露桡骨全长,显露桡骨近端1/3有损伤骨间后神经的危险。
但前路可以骨膜下剥离旋后肌,并用其来保护该神经,避免危险的发生。
同样,术中注意放置拉钩的位置,避免向后放置拉钩将神经直接压在桡骨上,因为骨间后神经可能在桡骨颈远端的桡骨粗隆对侧水平与骨直接接触。
这一入路首先为Henry所描述,故名Henry切口。
桡骨前侧入路的适应证如下:•1. 桡骨骨折切开复位和内固定术。
•2. 桡骨骨不连的植骨和固定术。
•3. 桡骨截骨术。
•4. 桡骨骨肿瘤的活检和治疗。
•5. 桡骨慢性骨髓炎的死骨摘除。
•6. 桡骨粗隆的前侧显露。
本节介绍一种显露桡骨全长的手术入路,通常仅根据需要而显露一部分。
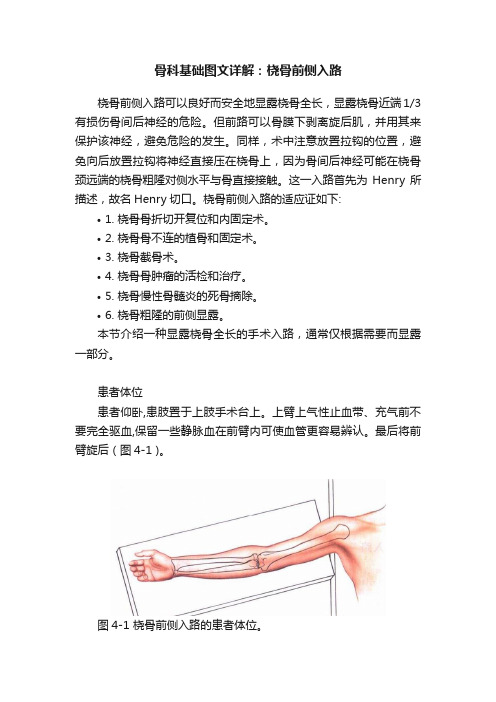
患者体位患者仰卧,患肢置于上肢手术台上。
上臂上气性止血带、充气前不要完全驱血,保留一些静脉血在前臂内可使血管更容易辨认。
最后将前臂旋后(图4-1 )。
图4-1 桡骨前侧入路的患者体位。
体表标志与切口# 体表标志肽二头肌腱该腱长而紧张,位于肘前肱桡肌内侧。
肱桡肌它是一块丰满的肌肉,与桡侧腕长、短伸肌共同起于肱骨外上银。
这3块肌肉构成“三合一活动块”、向下走行于旋后的前臂外侧。
桡骨茎突当手在解剖(旋后)位时,它位于桡骨外侧的最远端。
# 切口自肱二头肌腱外侧的肘屈侧皮肤横纹、向下直至桡骨茎突,作一直切口,切口长度视手术需要显露的程度而定(图4-2 )。
图4-2前臂前侧行一直切口,自肱二头肌外侧屈侧皮褶向下至桡骨茎突。
神经间平面远端神经间平面位于肱桡肌和桡侧腕屈肌之间,前者为桡神经支配,后者为正中神经支配(图4-3 )。
近端神经间平面位于肱桡肌和旋前圆肌之间,前者为桡神经支配,后者为正中神经支配。
图4-3 神经间平面。
此平面位于肱桡肌(桡神经)和桡侧腕屈肌(止中神经)之间。
浅层显露沿皮肤切口切开前臂深筋膜,找到下行的肱桡肌的内侧缘.在肱桡肌和桡侧腕屈肌之间打股平。
仕近端、这一平面位于旋前圆肌和肱桡肌之间(图4-4)。
前臂双骨折
前臂双骨折前臂双骨折重点难点掌握前臂双骨折的临床表现、诊断和治疗熟悉前臂解剖及骨折不同部位的移位方向了解前臂双骨折手术治疗方法一、概述·尺、桡骨干骨折(fracture of the radius and ulna )可由直接暴力、间接暴力、扭转暴力引起,有时导致骨折的暴力因素复杂。
·当单一尺骨或桡骨骨折时,暴力可由骨间膜传导到另一骨干,引起不同平面的双骨折,或发生一侧骨干骨折,另一骨的上端或下端脱位。
二、病因及分类1 .直接暴力多由于重物打击、机器或车轮的直接压榨,或刀砍伤,导致同一平面的横型或粉碎性骨折,由于暴力的直接作用,多伴有不同程度的软组织损伤,包括肌、肌腱断裂,神经血管损伤等。
2 .间接暴力跌倒时手掌着地,暴力通过腕关节向上传导,由于桡骨负重多于尺骨,暴力作用首先使桡骨骨折,若残余暴力比较强大,则通过骨间膜向内下方传导,引起低位尺骨斜形骨折。
3 .扭转暴力跌倒时手掌着地,同时前臂发生旋转,导致不同平面的尺桡骨螺旋形骨折或斜形骨折。
多为高位尺骨骨折和低位桡骨骨折。
三、临床表现和诊断·前臂出现疼痛、肿胀、畸形及功能障碍。
·检查可发现骨摩擦音及假关节活动。
骨传导音减弱或消失。
·X线平片检查应包括肘关节或腕关节,可发现骨折的准确部位、骨折类型及移位方向,以及是否合并有桡骨头脱位或尺骨小头脱位。
尺骨上1 / 3 骨干骨折可合并桡骨小头脱位,称为孟氏(Monteggia )骨折桡骨干下1 / 3 骨折合并尺骨小头脱位,称为盖氏(Galeazzi )骨折。
四、治疗1.保守治疗:手法复位外固定尺、桡骨骨干双骨折可发生多种移位,如重叠、成角、旋转及侧方移位等。
若治疗不当可发生尺、桡骨交叉愈合,影响旋转功能。
因此治疗的目标除了良好的对位、对线以外,特别注意防止畸形和旋转,力求达到解剖复位。
手法复位注意事项:在双骨折中,若其中一骨干骨折线为横形稳定骨折,另一骨干为不稳定的斜形或螺旋形骨折时,应先复位稳定的骨折,通过骨间膜的联系,再复位不稳定的骨折则较容易。
推荐-前臂双骨折的手术入路 精品
FCR
RADIAL ARTERY The radial artery may be taken in either direction, however, typically it is easier to take the artery to the radial side.
The deep dissection is now performed between the flexorpronator mass on the ulnar side and the artery and the mobile wad on the radial side.
After exposure of the volar aspect of the radius proximally and distally, two clamps can be placed on the ends of the bone in order to deliver them for cleaning.
尺桡骨双骨折
骨二科学习
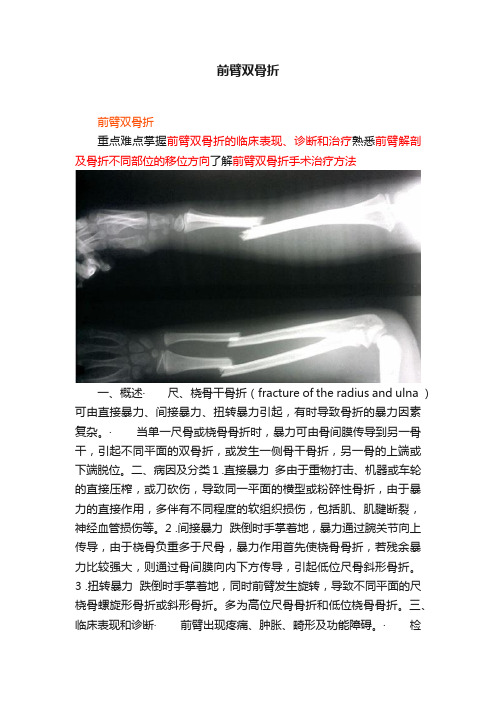
AP and lateral views of the both bones fracture of the forearm, demonstrating significant shortening and relatively simple oblique fracture patterns.
RADIAL ARTERY AND VENOUS COMMTANTES
A closeup of the distal aspect of the wound demonstrating The radial artery and its venous commtantes.
FCR
中医治疗前臂双骨折经验
中医治疗前臂双骨折经验前臂骨折是我们日常生活中比较常见的一种骨折,尤其是前臂双骨折更是比较常见。
传统的西医治疗方法主要是手术固定,但是手术后恢复时间较长,而且容易出现并发症。
中医治疗前臂双骨折也有着很好的效果,下面我将分享一些经验。
一、针灸治疗针灸治疗前臂双骨折可以缓解疼痛、消肿止血、促进骨折愈合。
常用的穴位有手太阴肺经的尺泽穴、手阳明大肠经的合谷穴等。
针灸治疗前臂双骨折需要注意穴位的选择和针刺的深度,一般需要在专业医师的指导下进行。
二、中药治疗中药治疗前臂双骨折主要是通过活血化瘀、消肿止痛、促进骨折愈合等作用来达到治疗的效果。
常用的中药有桃仁、红花、川芎等。
中药治疗前臂双骨折需要注意药物的剂量和煎药的方法,一般需要在专业医师的指导下进行。
三、推拿按摩推拿按摩可以促进局部血液循环,缓解疼痛、消肿止血、促进骨折愈合。
常用的推拿按摩手法有揉、捏、推、拿等。
推拿按摩治疗前臂双骨折需要注意手法的选择和力度的掌握,一般需要在专业医师的指导下进行。
四、食疗调理食疗调理可以通过调理身体内部环境来促进骨折的愈合。
常用的食疗有骨汤、牛奶、黑豆、花生等。
食疗调理需要注意食材的选择和烹饪的方法,一般需要在专业医师的指导下进行。
五、运动康复运动康复可以促进骨折愈合、恢复肌肉功能和关节活动度。
常用的运动有手指的活动、手腕的活动、前臂的旋转等。
运动康复需要注意运动的强度和频率,一般需要在专业医师的指导下进行。
综上所述,中医治疗前臂双骨折具有疗效显著、副作用小、恢复快等优点。
但是中医治疗前臂双骨折也有一定的局限性,如骨折严重、需要手术治疗等情况,建议及时就医。
早读创伤骨科最常用的手术入路大汇总,图示操作记忆更牢靠!

早读创伤骨科最常用的手术入路大汇总,图示操作记忆更牢靠!(1)肩部前方入路1)前侧入路(三角肌胸大肌间沟入路)1.切口:肩关节前方入路有两种切口。
•前方切口:沿三角肌胸大肌间隙10-15cm的切口,从喙突上方延长直达三角肌粗隆。
•腋路切口:起自腋前壁中点,朝后向腋后襞方向延长8-10cm,向上、外侧牵开皮瓣,显露三角肌胸大肌间沟。
2.神经界面:三角肌由腋神经支配;胸大肌由胸内、外神经支配。
3.注意事项:腋动脉由臂丛神经束包绕,位于胸小肌后方,喙突周围手术操作时,需内收上肢,以避免血管神经损伤。
肌皮神经在喙肱肌内侧,喙突下4-5cm进入并支配该肌,过度牵拉可引起肌皮神经麻痹。
显露并切开肩胛下肌时外旋手臂可增加肩胛下肌和腋神经距离,以保护腋神经。
2)肩锁关节和喙突入路(Roberts)切口:沿肩峰前上缘和锁骨外侧1/4作一弧形切口,再弯转向下沿三角肌胸大肌间沟下3-4cm。
3)肩关节前内侧入路(Thompson,Henry)适应症:关节盂前缘骨折合并肩锁关节周围的骨折脱位。
体位及术前准备:同前。
切口:始于肩锁关节的前上方,沿锁骨外1/2前缘向内侧走形,随后沿三角肌前缘向远端延伸,到该肌起点至止点的2/3处。
4)单纯喙突骨折的前侧微创入路切口:喙突外侧1cm作垂直切口,经三角肌胸大肌间沟进入或直接劈开喙突表面的三角肌纤维(2)后方入路1)后方入路(Judet入路)1.切口:始于肩峰尖的外侧,沿肩峰边缘向内后方延伸,弧形向远端走至肩胛下角2.神经界面:小圆肌(腋神经支配);冈下肌(肩胛上神经支配)之间3.注意事项•牵拉翻转三角肌时,不要用力过猛,以免损伤支配三角肌的腋神经(经四边孔支配小圆肌和三角肌)。
•在冈下肌和小圆肌之间分离后,将冈下肌向上牵开,注意保护肩胛上神经(经肩胛上切迹从冈上窝进入冈下窝,在冈下肌深面走形,支配冈下肌)2)简化的后方入路(King入路)1.切口:肩关节外展90°,在肩峰后方做垂直切口,并向下延伸10cm。
精彩继续一文详解桡骨前侧入路(HENRY入路)
精彩继续一文详解桡骨前侧入路(HENRY入路)桡骨前侧入路桡骨前侧人路可以良好而安全地显露桡骨全长、显露桡骨近端1/3有损伤骨间后神经的危险。
但前路可以骨膜下剥离旋后肌,并用其来保护该神经,避免危险的发生。
同样,术中注意放置拉钩的位置,避免向后放置拉钩将神经直接压在烧骨上,因为骨间后神经可能在桡骨颈远端的烧骨粗隆对侧水平与骨直接接触。
这一人路首先为Henry所描述,故名Henry 切口。
桡骨前侧入路的适应证如下:1.桡骨骨折切开复位和内固定术。
2,桡骨骨不连的植骨和固定术。
3.桡骨截骨术。
4.桡骨骨肿瘤的活检和治疗。
5,桡骨慢性骨髓炎的死骨摘除。
6,桡骨粗隆的前侧显露。
The biceps brachii is a muscle in the upper arm. It is located in the upper part of the humerus and is part of the muscle network in the arm along with muscles such as the brachialis and brachioradialis. The biceps brachii is a compound muscle made up of two heads: the long head and the short head. They originate from the upper and lower heads of the humerus, respectively, and end at the lower part of the humerus. The main function of the biceps brachii is to flex and rotate the elbow joint, whether the elbow is extended or flexed. It also helps to support and stabilize the wrist. Damage or strain to the biceps brachii can limit elbow movement and affect hand function. Physical therapy and rehabilitation exercises can help to restore muscle function.biceps brachii(肱二头肌)是人体上肱部的一种肌肉。
新技术—掌侧入路治疗前臂双骨折,更快捷,更安全!

新技术—掌侧入路治疗前臂双骨折,更快捷,更安全!01前言目前前臂骨折多选择切开复位内固定治疗。
本研究笔者介绍了一种改良前臂掌侧入路。
采用掌侧单切口显露2个操作窗口来显露前臂的内外侧腔室。
不仅能够避免骨间膜异位骨化的发生,而且对周围的血管神经损伤较小。
该入路主要适用于复杂的桡骨远端骨折和尺骨干骨折。
02入路介绍患者仰卧位,神经丛阻滞麻醉,上止血带。
选择掌侧入路,腕横纹近端1cm切开,术中根据骨折部位可平行掌长肌向近端延伸扩大切口。
依次切开皮下和筋膜,于FCR(桡侧腕屈肌腱)和PL(掌长肌)间隙进入,通过单一切口双窗口显露尺桡骨(内侧尺骨窗,外侧桡骨窗)。
术中需要综合考虑前臂、肘关节和尺桡关节,前臂双骨骨折需要解剖复位,以免影响前臂旋转功能。
虽然大多数长骨骨干骨折可以选择弹性髓内钉固定,但笔者建议选择加压钢板螺钉进行坚强固定,可以获得直接愈合。
对于前臂粉碎性骨折最好选择弹性固定,缺点是间接愈合会有骨痂形成,导致前臂旋转受限。
选择掌侧或背侧钢板尚存在争议,有报道认为背侧钢板会引起肌腱炎,甚至导致伸肌腱断裂。
而掌侧钢板可能会引起撞击综合征。
依据我们的经验将钢板置于尺桡骨掌侧,可以获得良好的软组织覆盖。
术中首先处理简单骨折,以恢复长度和力线,避免旋转受限。
01 外侧(桡骨)窗将FCR、桡动脉和肱桡肌向桡侧牵开,指浅屈肌腱(FDS)、拇长屈肌腱向尺侧牵开以保护正中神经(见图2所示)。
随后切开旋前方肌显露桡骨近端。
前臂近端骨折显露时,可以将前臂置于旋前位,显露并掀起旋前圆肌,以便更好地显露桡骨近端。
图1所示。
A和B. 前臂双骨折正侧位片。
C和D. 术中透视显示骨折复位和内固定情况。
E. 术后3个月手术瘢痕。
图2所示。
桡侧窗:桡肱肌(a)、桡动脉(b)、桡骨(c)、拇长屈肌(d)、桡侧腕屈肌(e)、掌长肌(f)。
02 内侧(尺骨)窗由尺侧腕屈肌腱FCU(尺神经支配)和指浅屈肌腱(FDS)(正中神经支配)肌间隙进入。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
A useful technique to make the skin incision is to take a bovi cord and pull it taught from the radial side of the biceps tendon to the FCR at the level of the wrist. This can then be used as a template for the incision line.
FDS
The pronator is being released from the radial aspect of the radius in a subperiosteal manner. This subperiosteal dissection continues distally to release the origin of the common flexor.
The following sequence demonstrates using the offset drill guide to place an eccentrically drilled hole away from the fracture. The screw is placed to the point where it abuts but is not inserted completely within the plate until it is affixed on the other side.
FCU
FLEXOR CARPI ULNARIS
ECU
EXTENSOR CARPI ULNARIS
These figures demonstrate reduction of the fracture with a plate held in place on the flat, volar aspect of the bone. Once the reduction is confirmed fixation of the plate is performed using a compressive technique through the plate.
尺桡骨双骨折
骨二科学习
AP and lateral views of the both bones fracture of the forearm, demonstrating significant shortening and relatively simple oblique fracture patterns.
RADIAL ARTERY AND VENOUS COMMTANTES A closeup of the distal aspect of the wound demonstrating The radial artery and its venous commtantes.
FCR
RADIAL ARTERY The fascia on the radial side of the flexor carpi radialis is released, exposing the deep tissue. The radial artery can be followed now throughout the entire incision.
FCR
RADIAL ARTERY Each side of the fracture is be delivered in order to expose and clean the cortical edges.
These figures demonstrate delivery of the distal fragment and a curved curette being used to clean the cortical edge. No cleaning should be performed within the intramedullary canal,as this is healthy tissue and can be useful for the healing process.
RADIAL ARTERY
BICEPS TENDON
FLEXOR CARPI RADIALIS (FCR)
The patient is positioned supine with the arm prepped and draped to just above the elbow and a tourniquet in place. This figure demonstrates the arm held in supination. Note the position of the biceps insertion as well as the palpable tendon of the FCR and radial artery.
FCR RADIAL ARTERY
The incision is taken down through the skin, identifying the fascial layer with care taken not to damage any superficial veins that may be intact. The FCR tendon is clearly visible throughout the wound, as is the radial artery in the distal extent of the wound.
Once the fractures are completely cleaned along their cortical edges such that the fracture reduction can be visualized, the two clamps are used to reduce the fracture. If a butterfly fragment exists, it is necessary to fix this with a lag screw back to one of the fracture ends in order to realign the fracture.
PRONATOR For the proximal dissection, the forearm is brought into supination and the pronator, FDS and FDP are released from the volar aspect of the radius
HOLE ECCENTRICALLY ILLUSTRATED
In a similar fashion to the first screw, the second screw is placed on the opposite side of the fracture, also eccentrically away from the fracture. By compressing these two screws against the plate the fracture is translated and compressed together as shown in the following sequence.
FCR
RADIAL ARTERY
The radial artery may be taken in either direction, however, typically it is easier to take the artery to the radial side.
The deep dissection is now performed between the flexorpronator mass on the ulnar side and the artery and the mobile wad on the radial side.
In the current case, the fracture is a simple pattern and is reduced by delivering the bones jointly, accentuating the deformity and then rotating and fitting the bones together with progressive compression while pushing the bones back into the wound, obtaining alignment by steric interference of one side against the other.
After exposure of the volar aspect of the radius proximally and distally, two clamps can be placed on the ends of the bone in order to deliver them for cleaning.
Once the bones are held reduced, as seen in the following sequence, an appropriate dynamic compression plate is placed and held in place with a clamp. It is important that this plate must have the appropriate bend for the volar aspect of the forearm so as not to gap open the dorsal side as the plate is fixed to the bone. Thus, it should be slightly underbent with respect to the standard volar concavity.